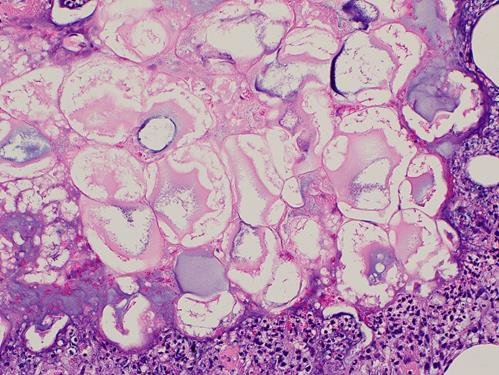
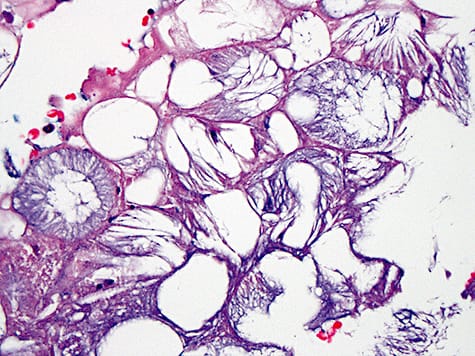
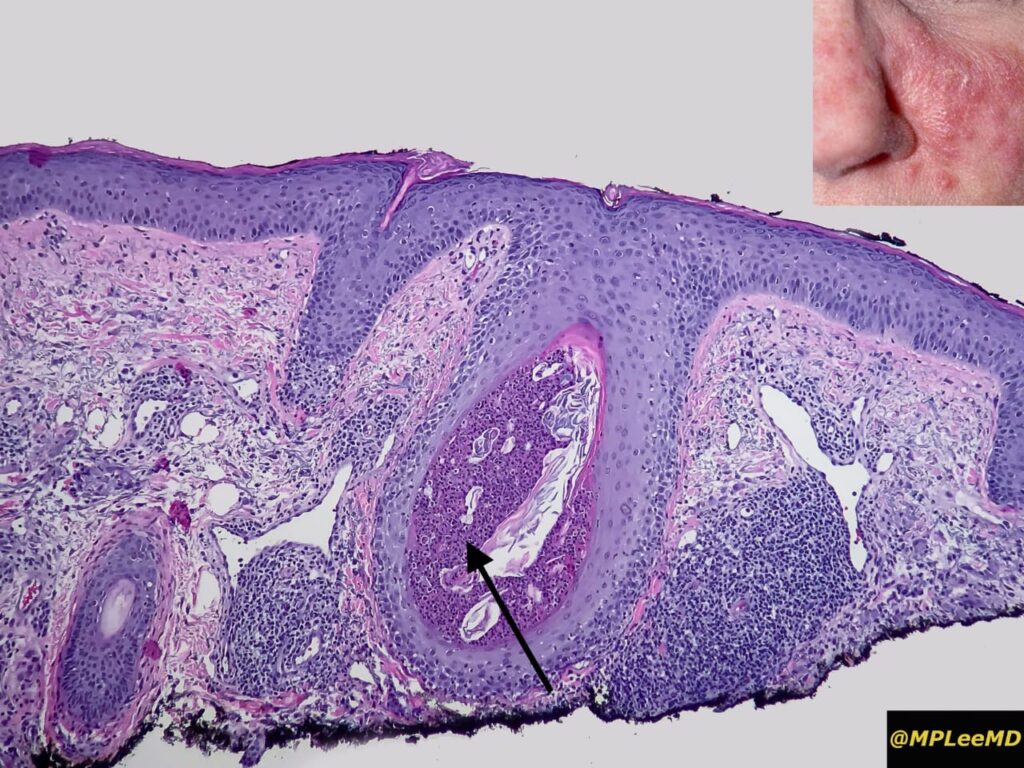
mostly these are *matrix naevi* leading to band, so focal matrix ablation might lead a nail plate dystophy lateron which might look uglier than this
Would the nail appearance be normal after this procedure and complete healing?
*Yes only the transverse lenght* *will be shortened* , rest it will be perfact
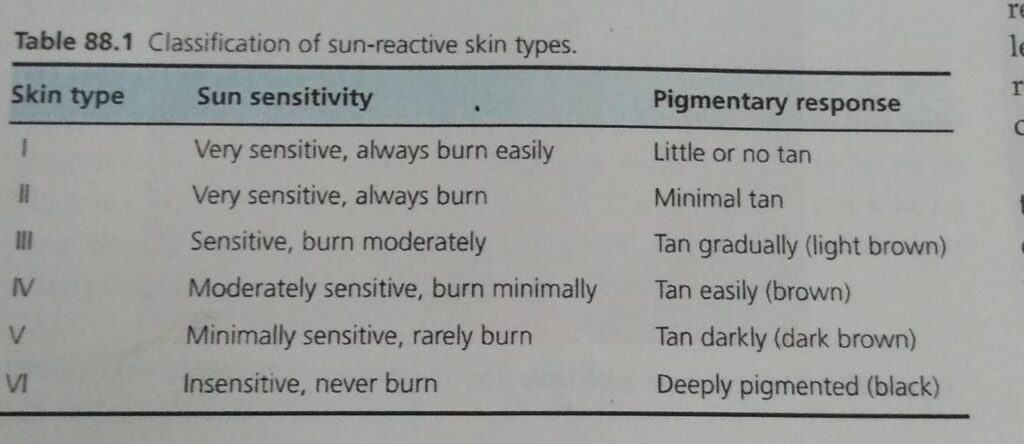
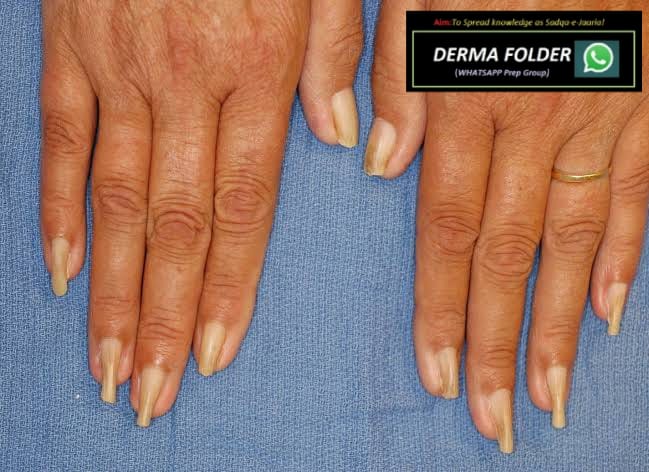
Grabbing this opportunity to revise *ABCDEFGHI* , to R/O *subungual melanoma* in such cases
*A: Age (* 50–70 years old); African, Japanese, Chinese, and Native American heritage
*B: Brown-black* pigmented band ≥3mm with blurred borders
*C: Change or lack of change* despite treatment in the nail band or nail morphology
*D: Digit most* commonly involved (thumb, big toe, or index finger)
*E: Extension* of pigment into the skin surrounding the nail (Hutchinson sign)
*F: Family or personal history* of melanoma or dysplastic nevus (atypical mole)
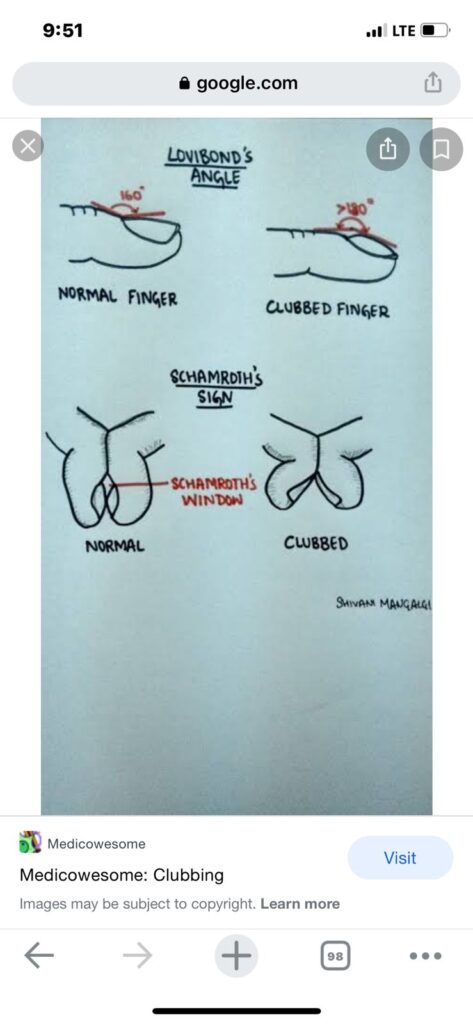
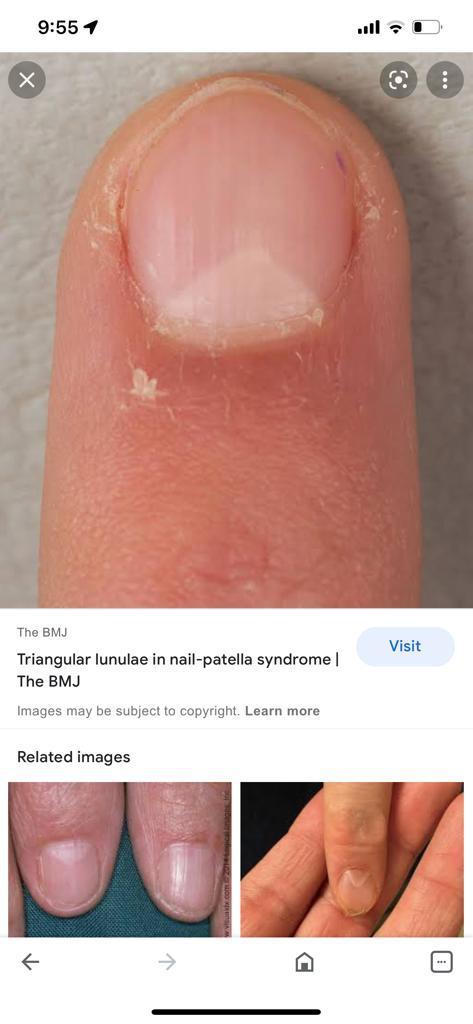
*G – Geometry* of lesion like triangular band
*H – Hyponychial involvement*
*I – irregular pigment pattern* (like different color bands) , irregular spaces , irregular thickness


































































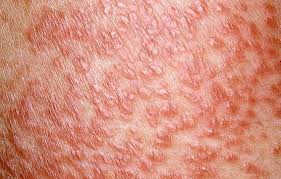
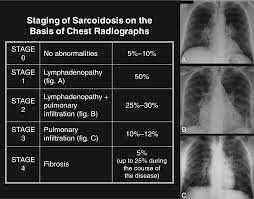
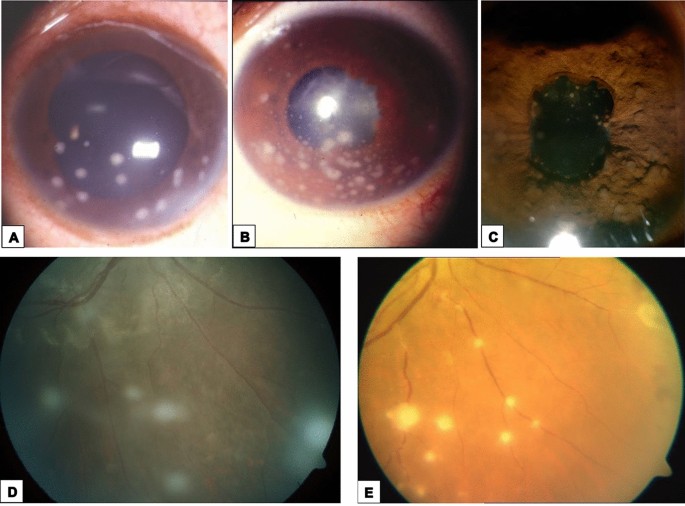
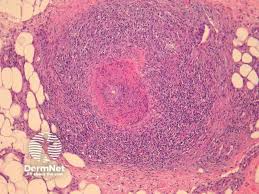
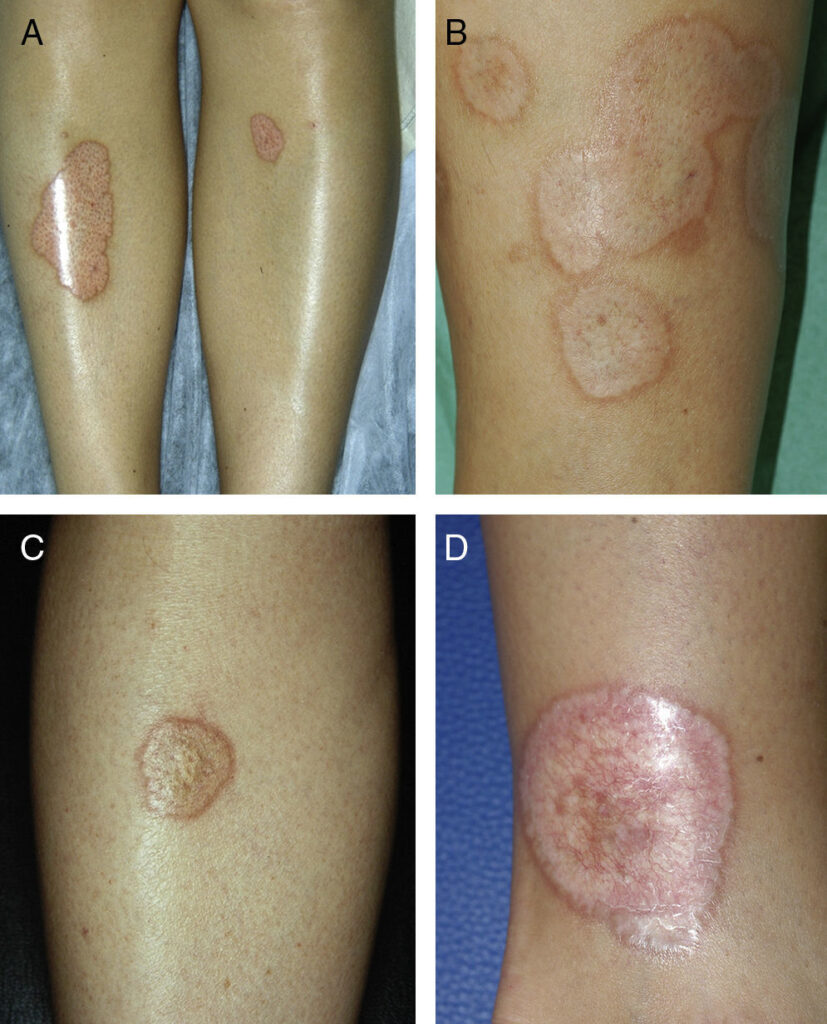
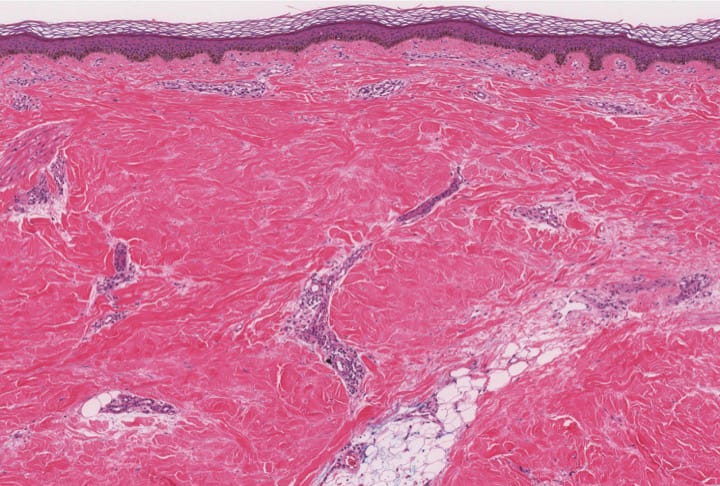
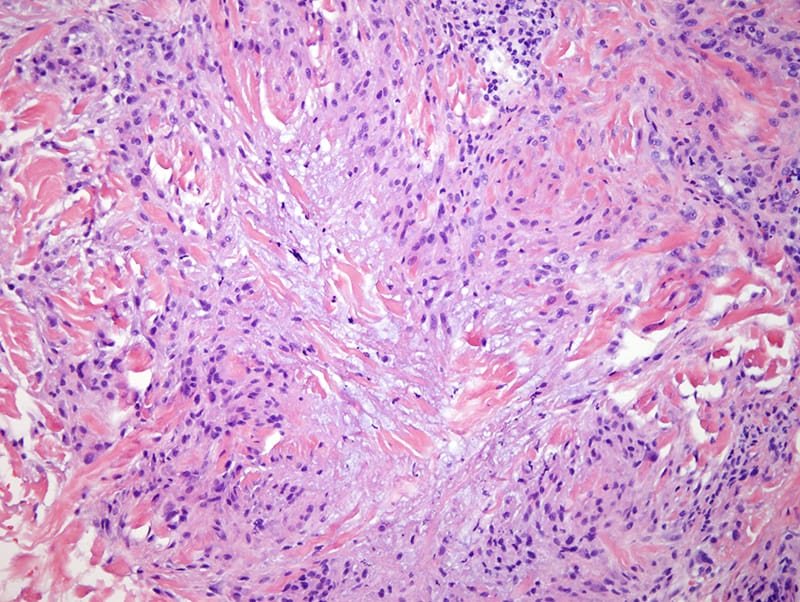
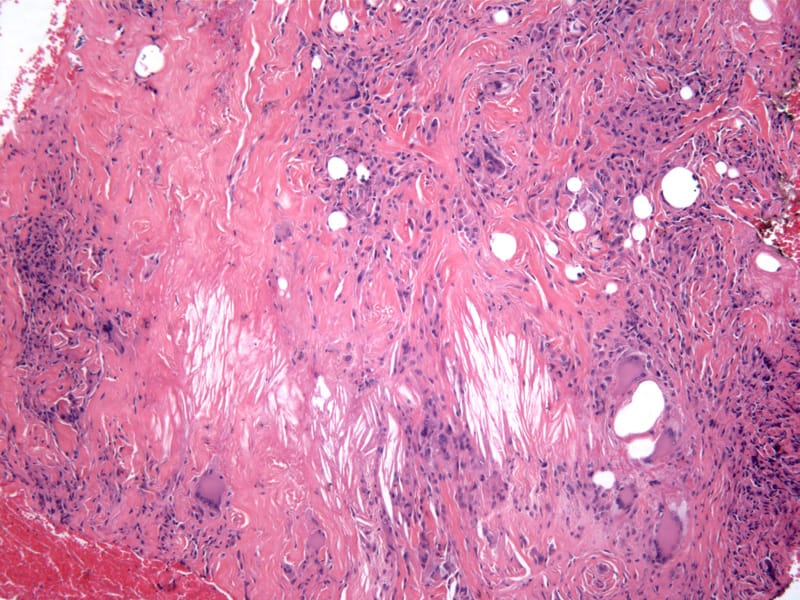
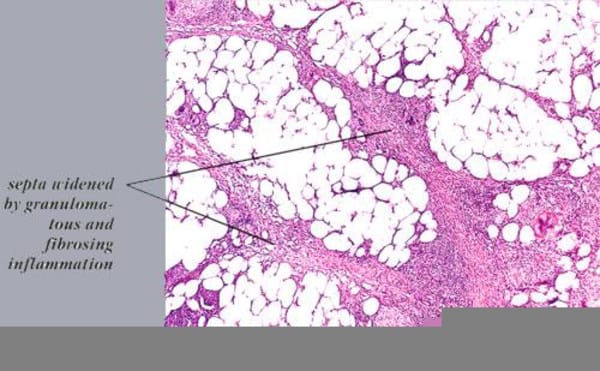
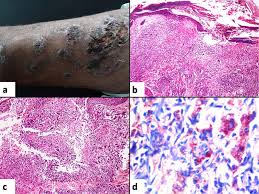
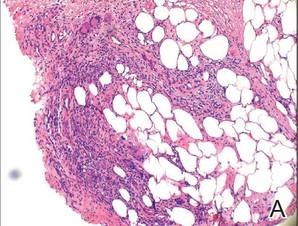
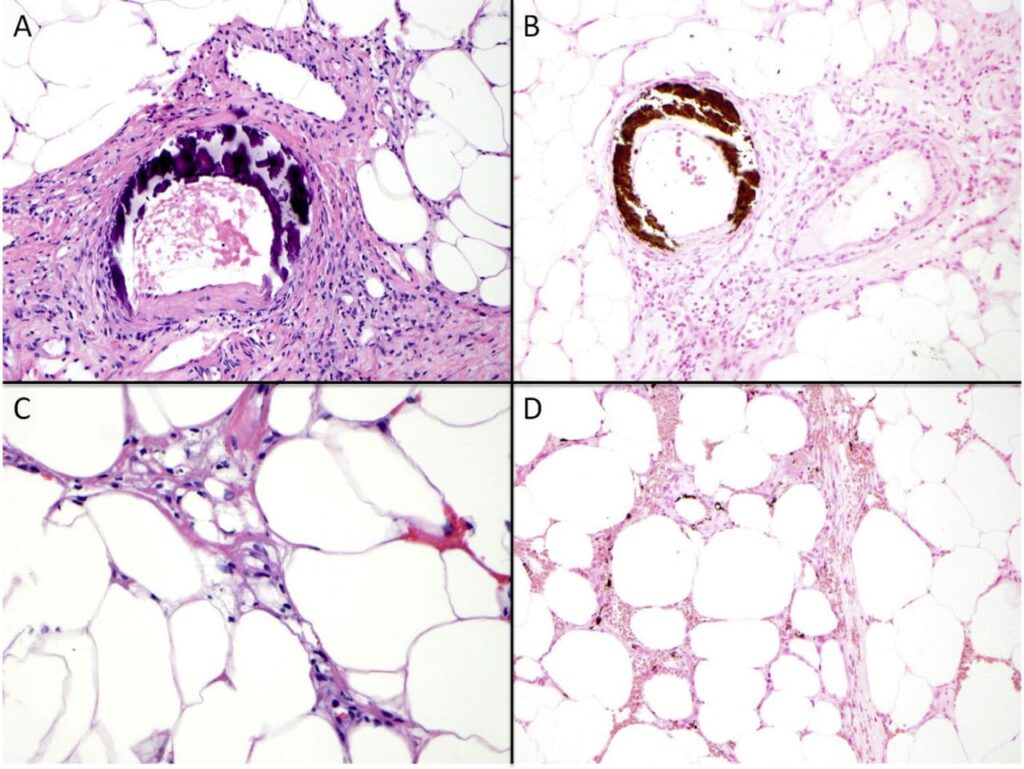
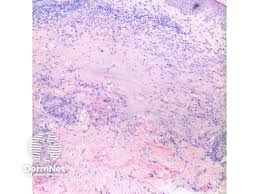
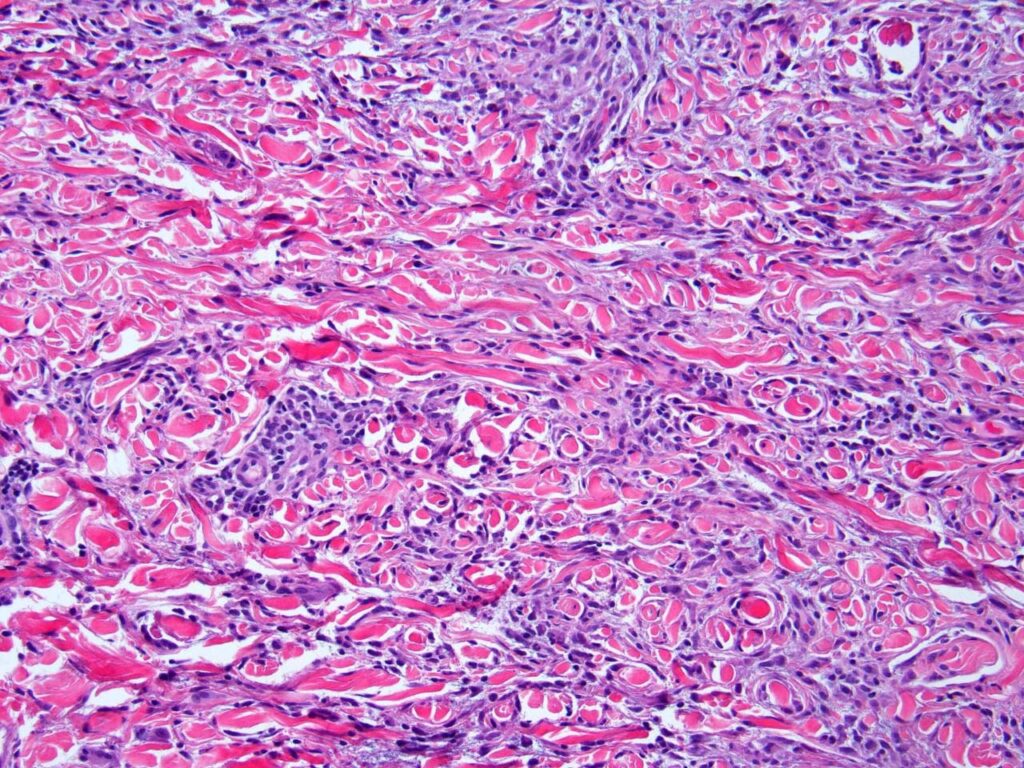
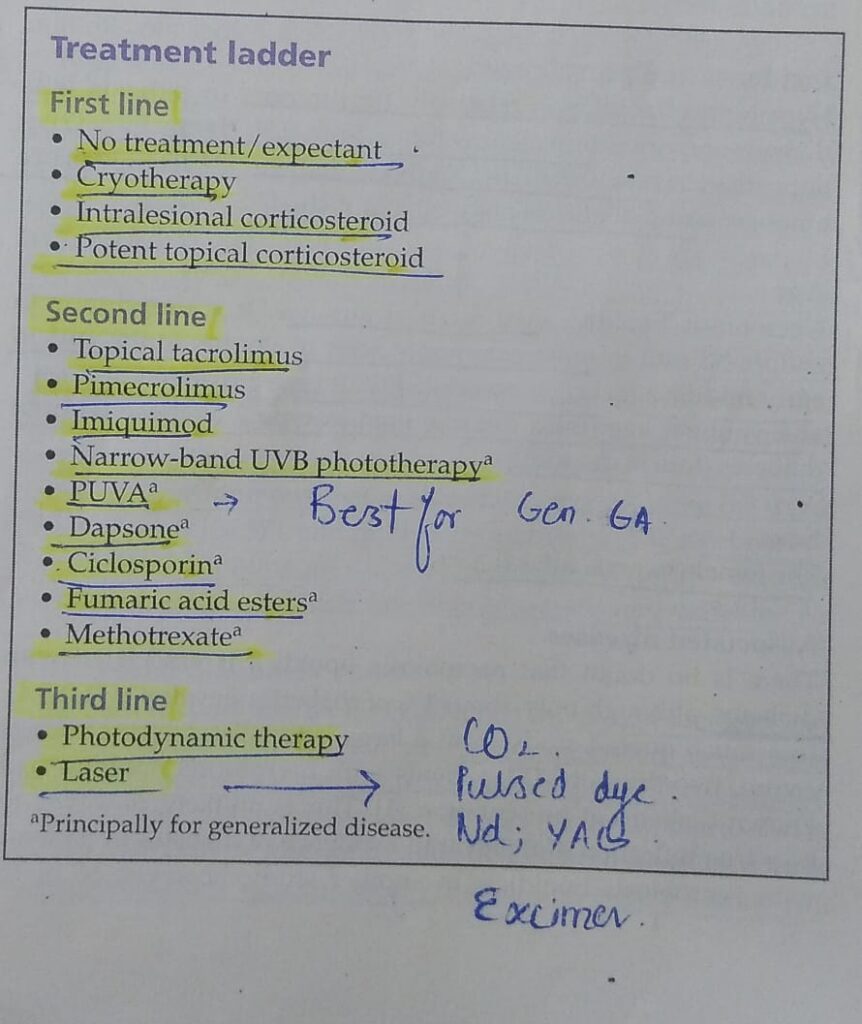
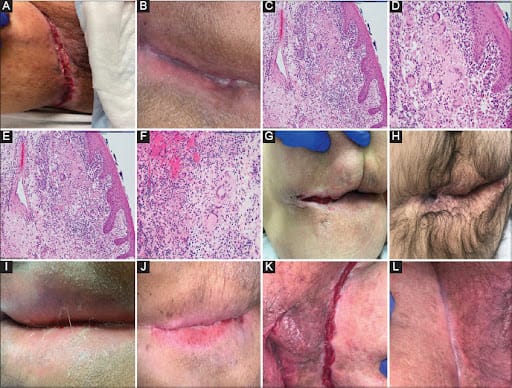
 *SARCOIDOSIS*
*SARCOIDOSIS*