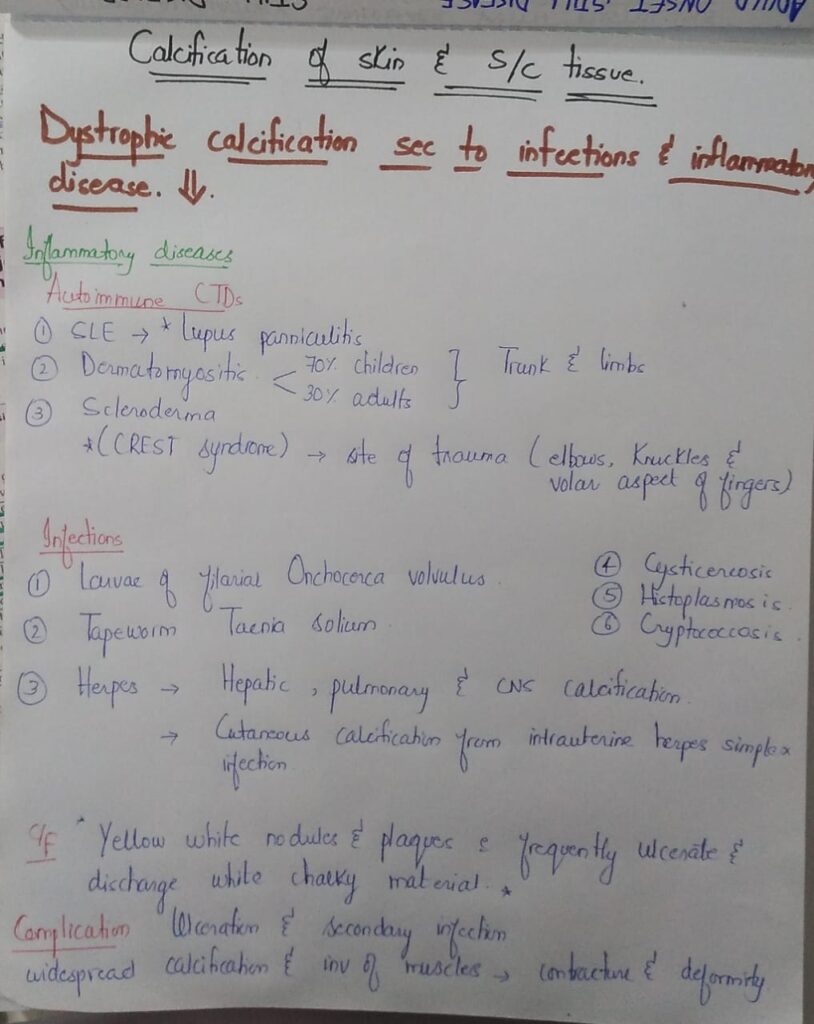

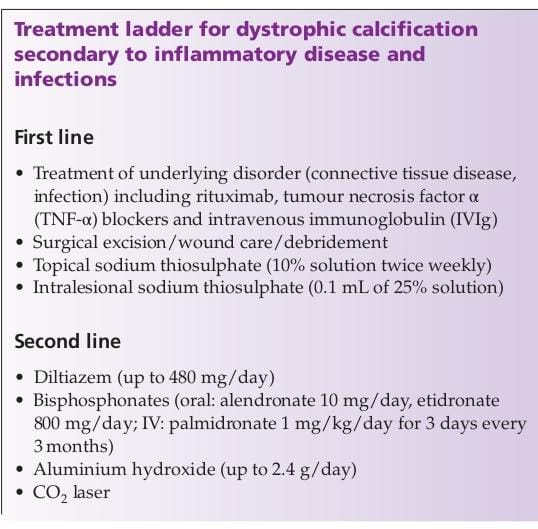



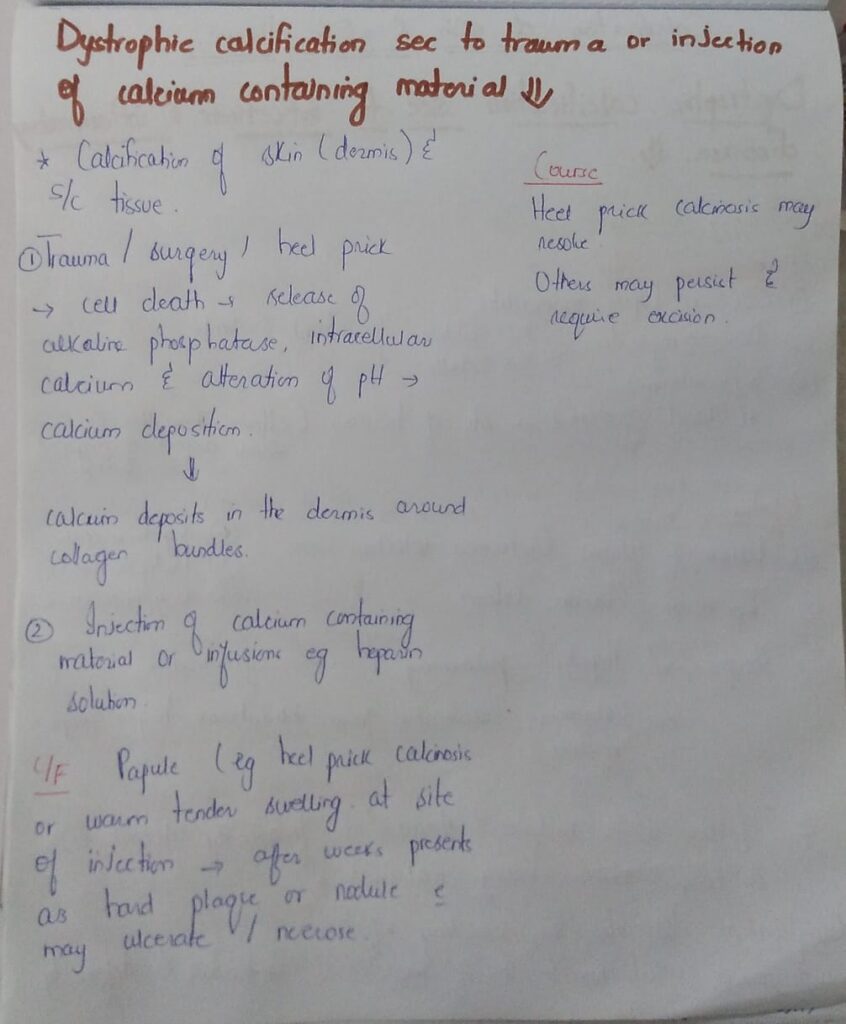
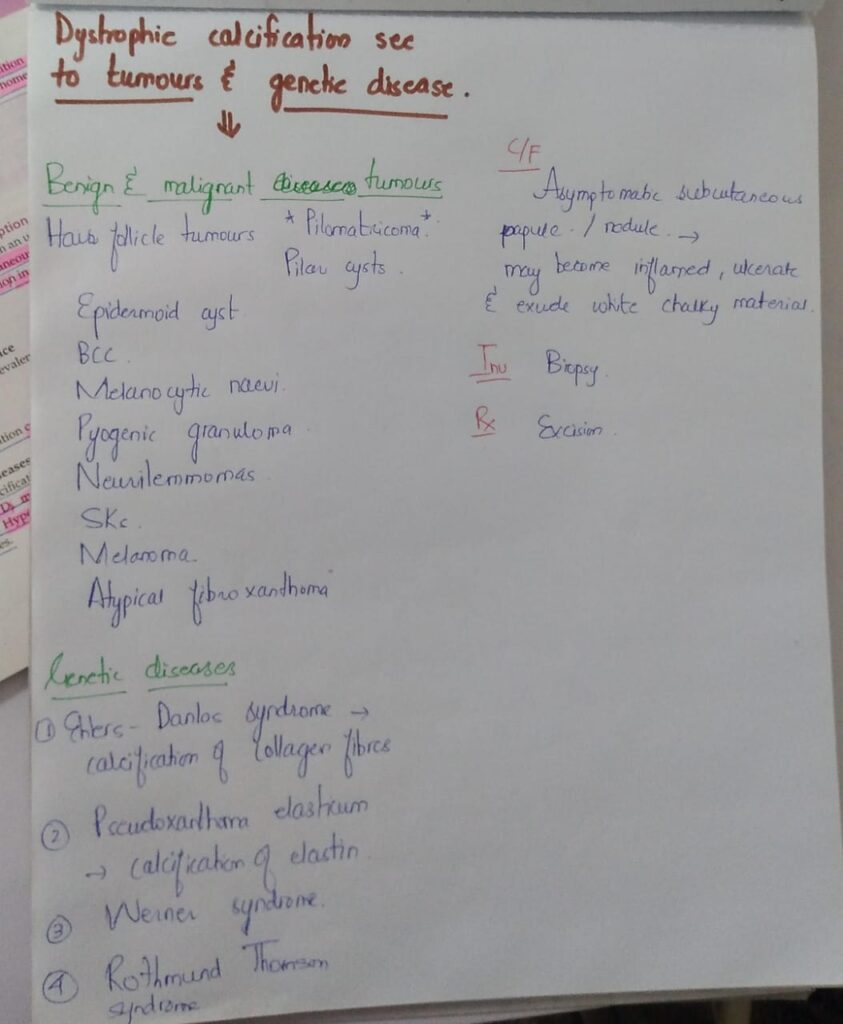
Calcinosis cutis 
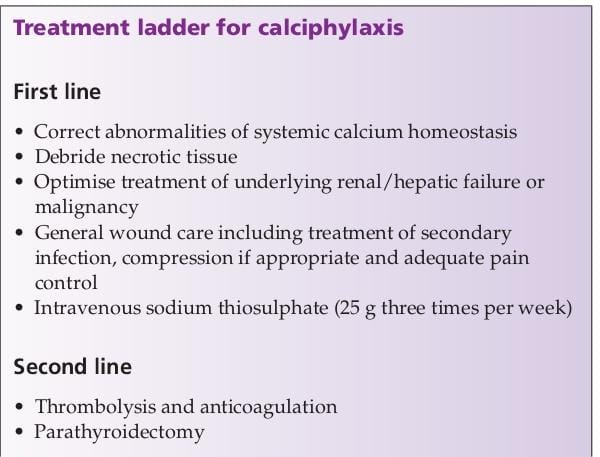
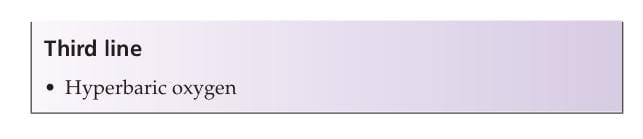
 Calciphylaxis
Calciphylaxis


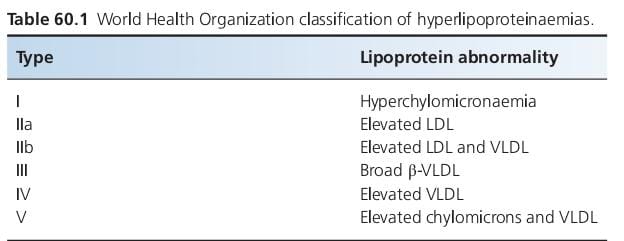









Primary dyslipidaemias; Combined dyslipidaemias
Primary dyslipidaemias; Hypertriglyceridaemias
With these 2, u ll need only 15 mins to revise this boring chap.
Happy learning
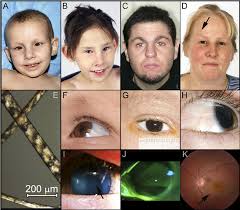
*Cerobrotendinous xanthomatosis*
 Autosomal recessive
Autosomal recessive
Defect in Sterol 27 hydroxylase
Inc levels of Cholestenol and 7 hydroxycholesterol.
Plasma cholesterol levels are normal
Childhood or earlyadulthood
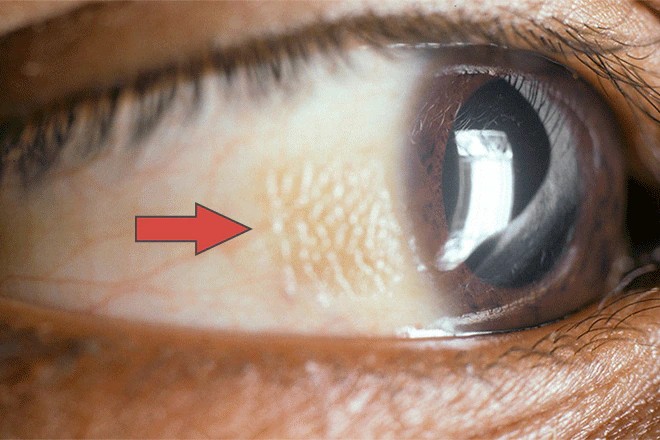
Tendon xanthomas and xanthelasmas
Myelin destruction in CNS due to accumulation of cholestenol and 27 OH cholesterol leading to mental retardation, seizures,spasticity, ataxia, peripheral neuropathy.
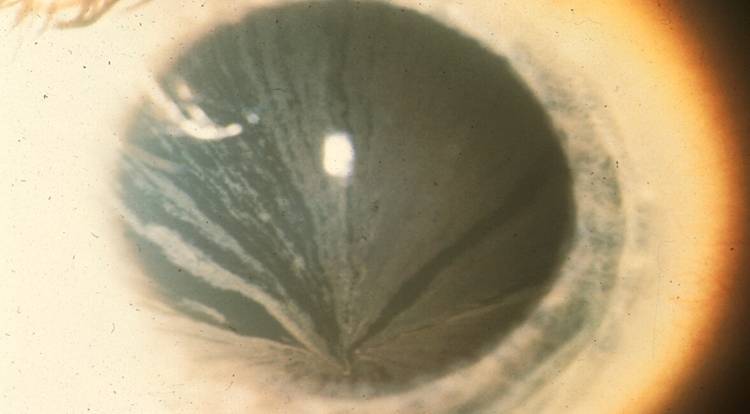
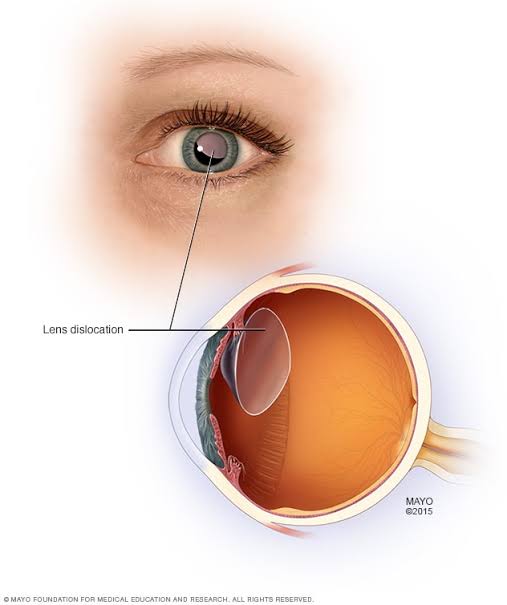
Early onset cataract
Diarrhea
Premature osteoprosis
Inc risk of CVD
TREATMENT
Chenodeoxycholate
*Sitosterolaemia*
️Autosomal recessive
️ABCG5 and ABCG8 mutation
️Defect in proteins Sterolin-1 and Sterolin-2 in enterocytes and hepatocytes.
These transport plant sterols to facilitate their excretion.
Defects leads to raised levels of plant sterols ” Beta sitosterol” in body
️Impaired growth
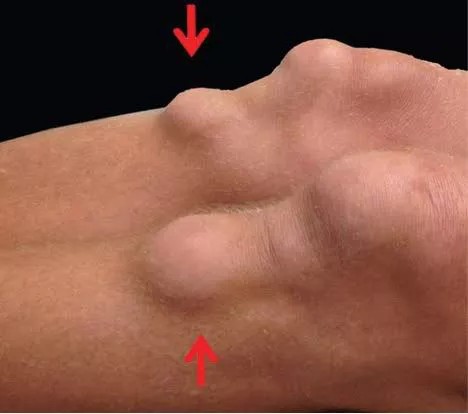
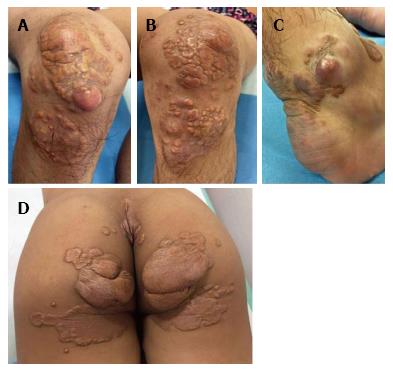
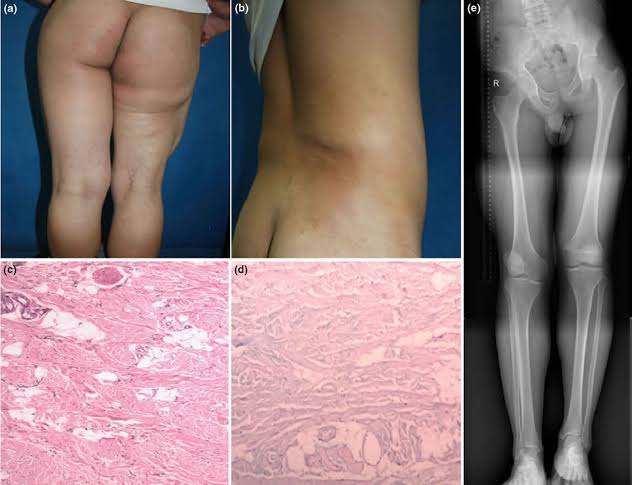
Tendon xanthomas
Tuberous xanthomas
Anaemia and thrombocytopenia
Arthritis
Inc risk of premature CVD
️Treatment
*Ezetimibe* reduces plant sterol levels
*Secondary dyslipidaemias*
1️⃣ Diabetes mellitus
Type I Increased HDL, LDL and VLDL and hence increased risk of CVD
Type II Decreased HDL, Normal LDL and Increased Tgs.
2️⃣ Chronic cholestasis
Increased Cholesterol
3️⃣Nephrotic syndrome
Increased cholesterol
4️⃣ Chronic renal failure
Increased Tgs
5️⃣Alcohol
Increased Tgs
6️⃣Systemic steroids
Increased LDL and HDL
7️⃣ Ciclosporin
Increased LDL cholesterol
8️⃣ Retinoic acid deriavatives
Increased Tgs
Primary dyslipidaemias; Combined dyslipidaemias
Primary dyslipidaemias; Hypertriglyceridaemias
With these 2, u ll need only 15 mins to revise this boring chap.
Happy learning
*Cerobrotendinous xanthomatosis*
Autosomal recessive
Defect in Sterol 27 hydroxylase
Inc levels of Cholestenol and 7 hydroxycholesterol.
Plasma cholesterol levels are normal
Childhood or earlyadulthood
Tendon xanthomas and xanthelasmas
Myelin destruction in CNS due to accumulation of cholestenol and 27 OH cholesterol leading to mental retardation, seizures,spasticity, ataxia, peripheral neuropathy.
Early onset cataract
Diarrhea
Premature osteoprosis
Inc risk of CVD
TREATMENT
Chenodeoxycholate
*Sitosterolaemia*
️Autosomal recessive
️ABCG5 and ABCG8 mutation
️Defect in proteins Sterolin-1 and Sterolin-2 in enterocytes and hepatocytes.
These transport plant sterols to facilitate their excretion.
Defects leads to raised levels of plant sterols ” Beta sitosterol” in body
️Impaired growth
Tendon xanthomas
Tuberous xanthomas
Anaemia and thrombocytopenia
Arthritis
Inc risk of premature CVD
️Treatment
*Ezetimibe* reduces plant sterol levels
*Secondary dyslipidaemias*
1️⃣ Diabetes mellitus
Type I Increased HDL, LDL and VLDL and hence increased risk of CVD
Type II Decreased HDL, Normal LDL and Increased Tgs.
2️⃣ Chronic cholestasis
Increased Cholesterol
3️⃣Nephrotic syndrome
Increased cholesterol
4️⃣ Chronic renal failure
Increased Tgs
5️⃣Alcohol
Increased Tgs
6️⃣Systemic steroids
Increased LDL and HDL
7️⃣ Ciclosporin
Increased LDL cholesterol
8️⃣ Retinoic acid deriavatives
Increased Tgs



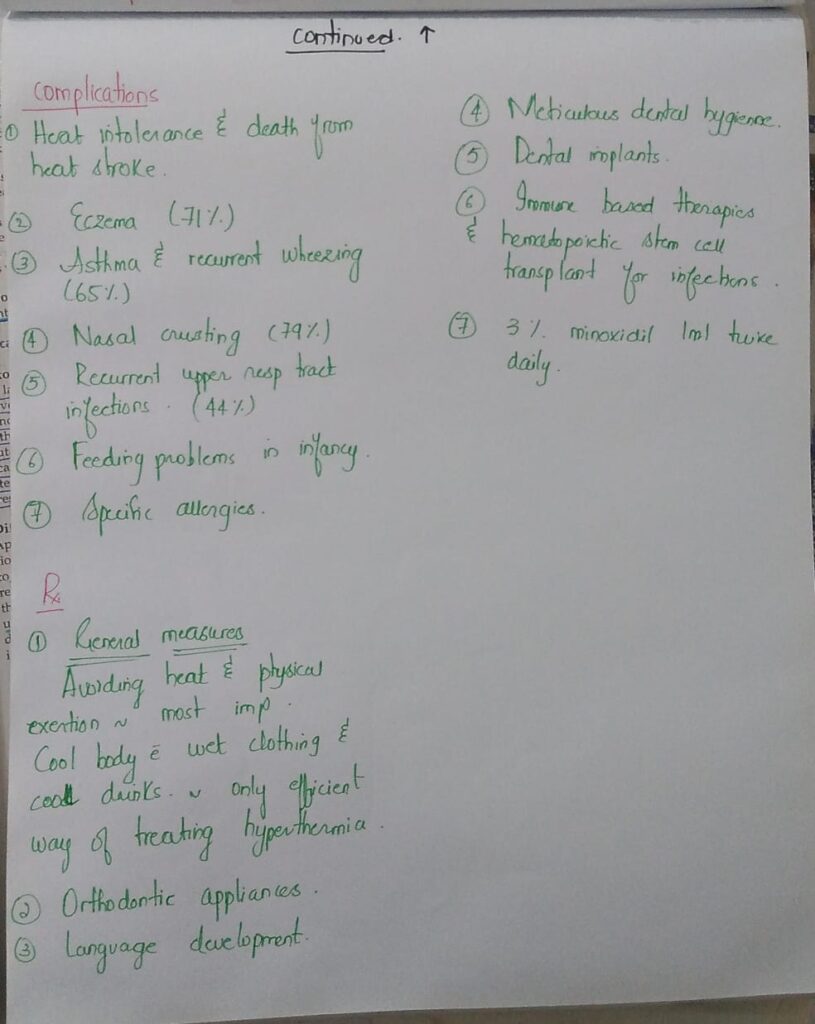
Vitamins deficiency / excess
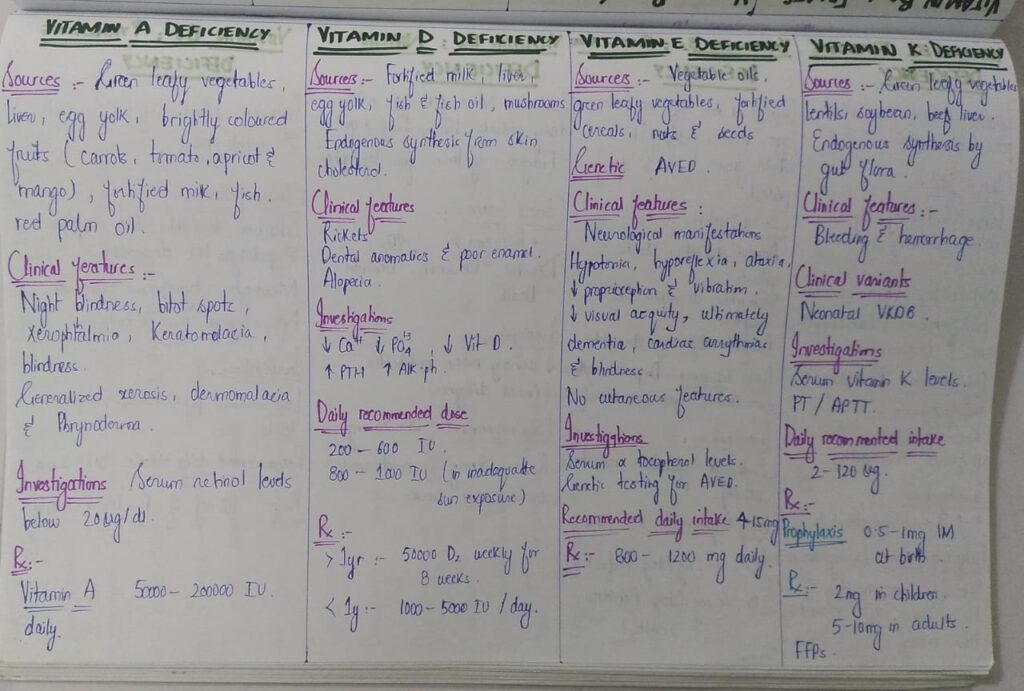
Vitamin A deficiency

Vitamin A excess

Vitamin D deficiency
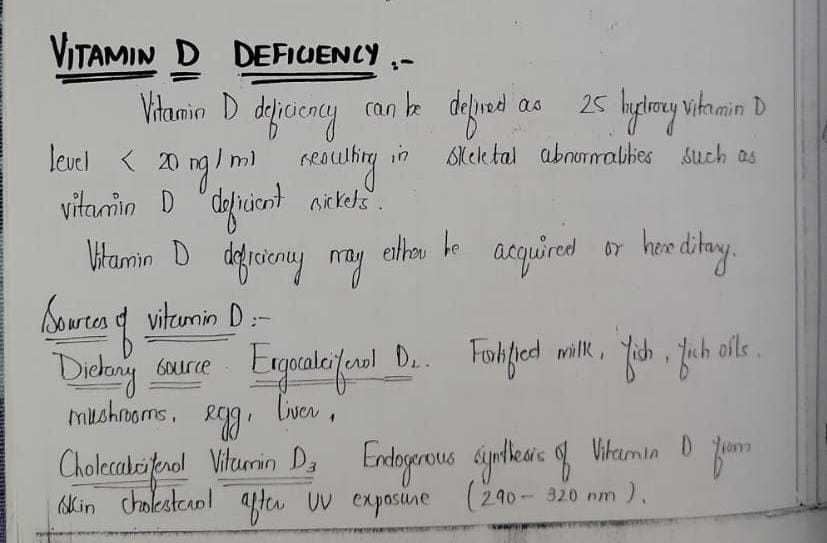
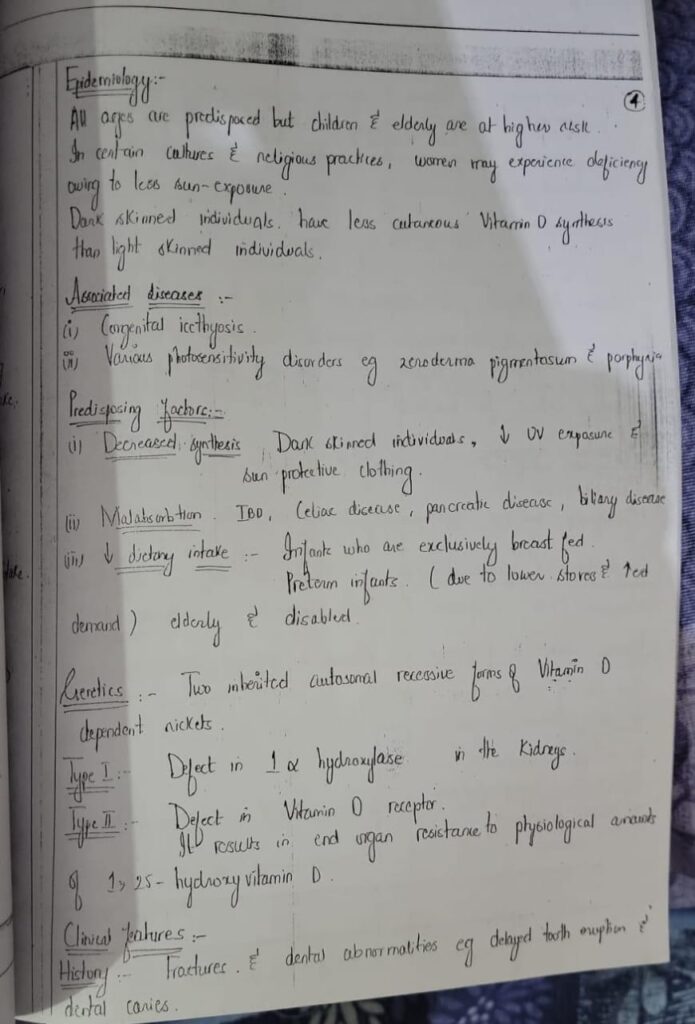

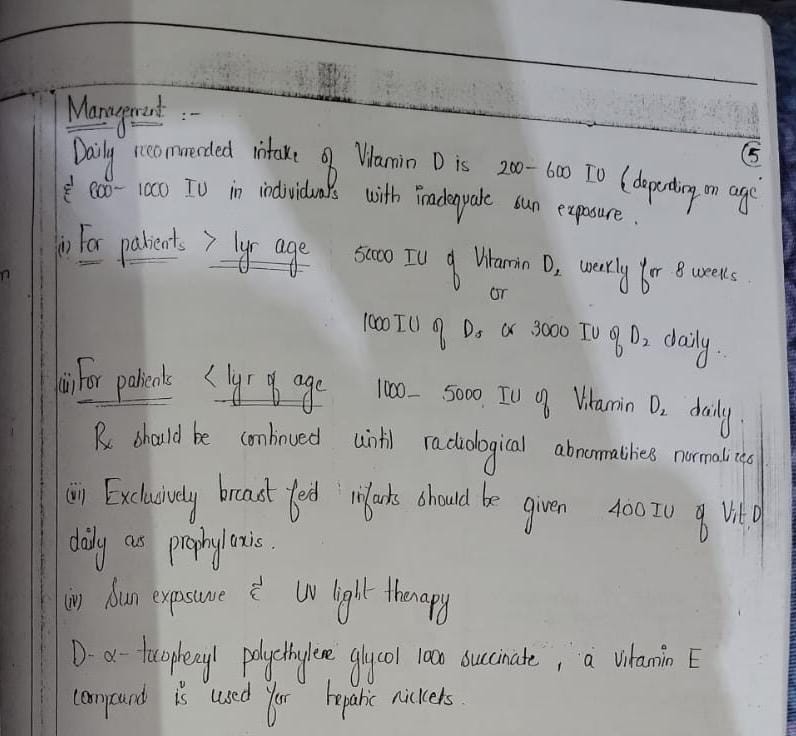
For vitamin D, read from above and then revise from mcqs only
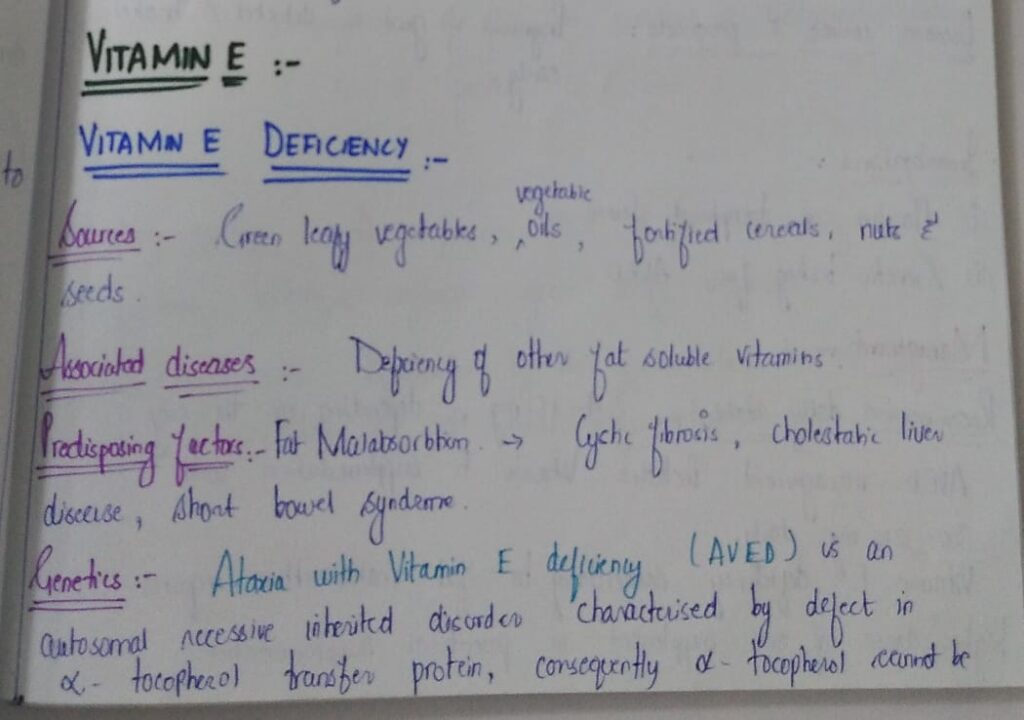
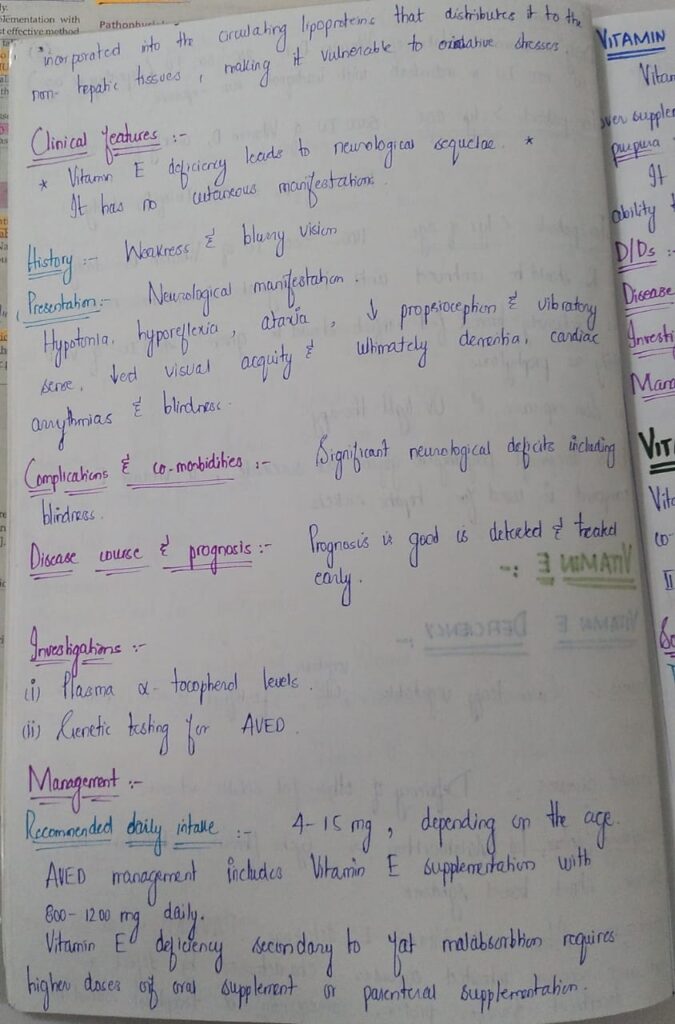
Vitamin E deficiency
Vitamin E excess




Read from above and revise with solving mcqs only
IMPORTANT TIP
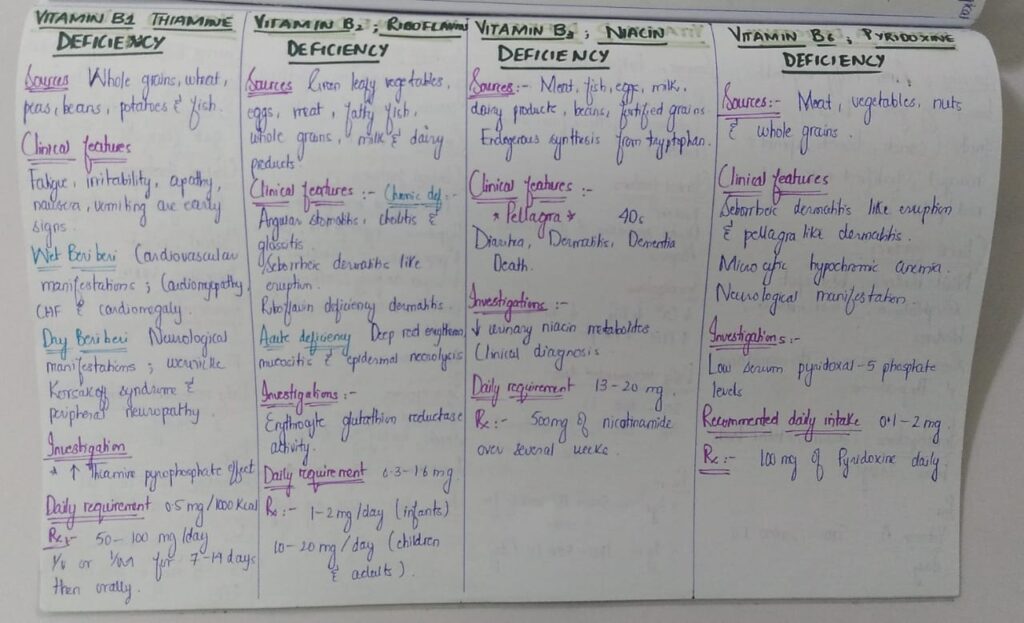
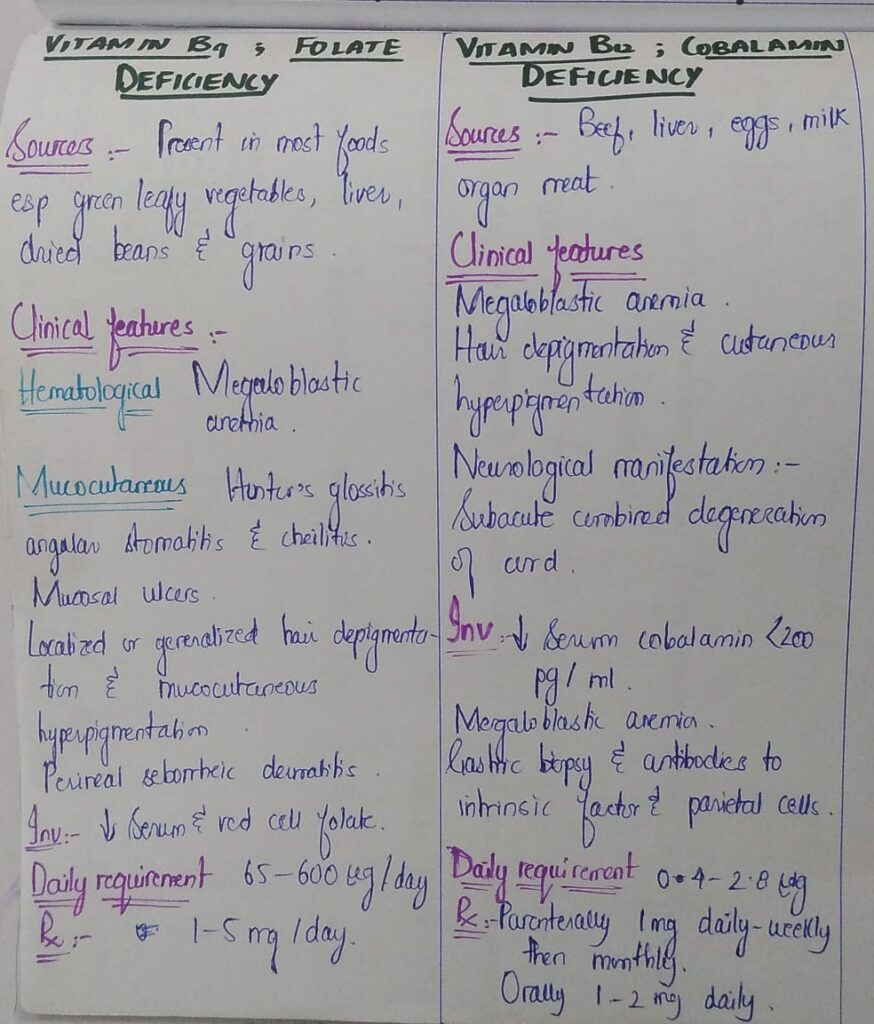
 Water soluble vitamins
Water soluble vitamins





Vitamin C deficiency














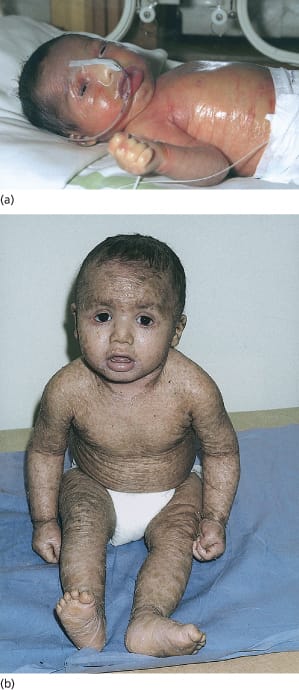
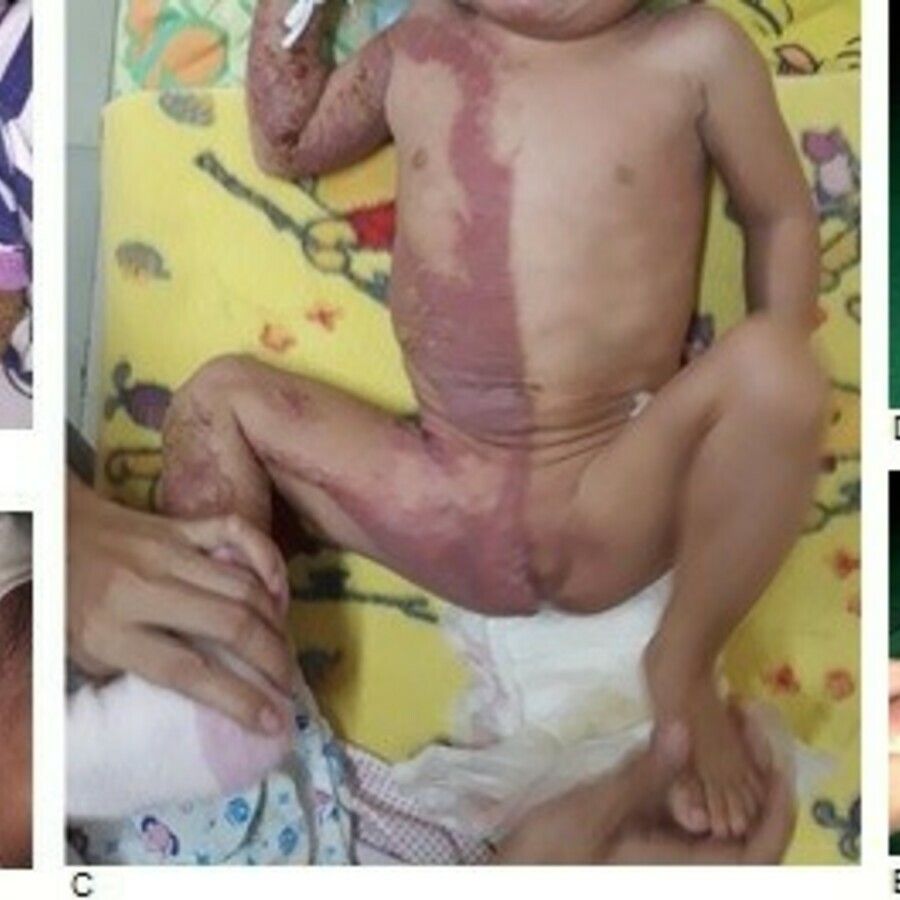
AUTOSOMAL RECESSIVE CONGENITAL ICHTHYOSIS
1. Harlequine ichthyosis

Collodion baby and self improving congenital ichthyosis
Bathing suit ichthyosis

Lamellar ichthyosis and Congenital ichthyosiform erythroderma







KERATINOPATHIC ICHTHYOSIS

























































































































































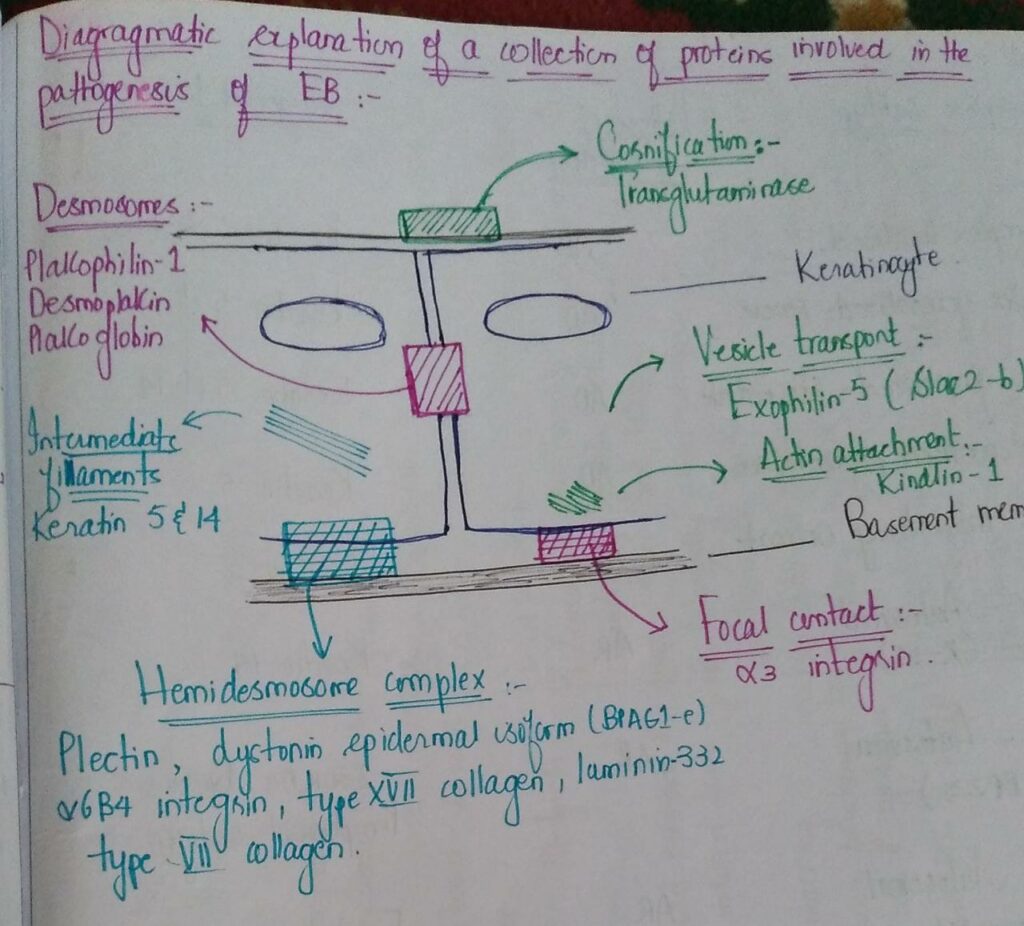

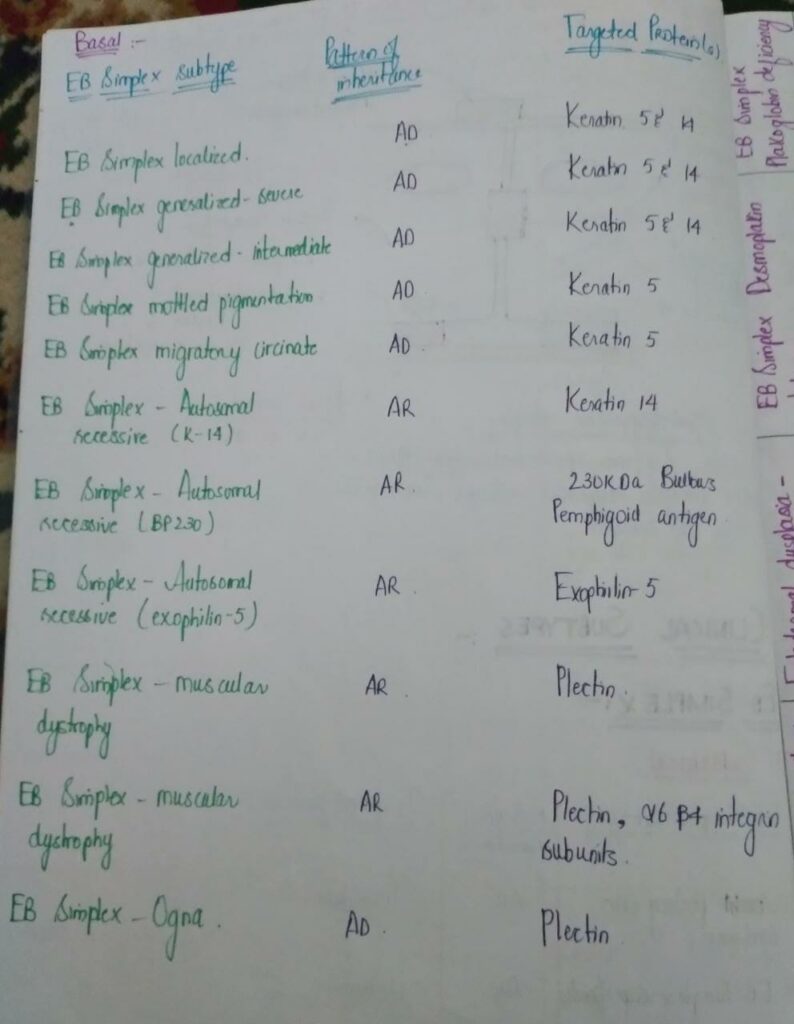



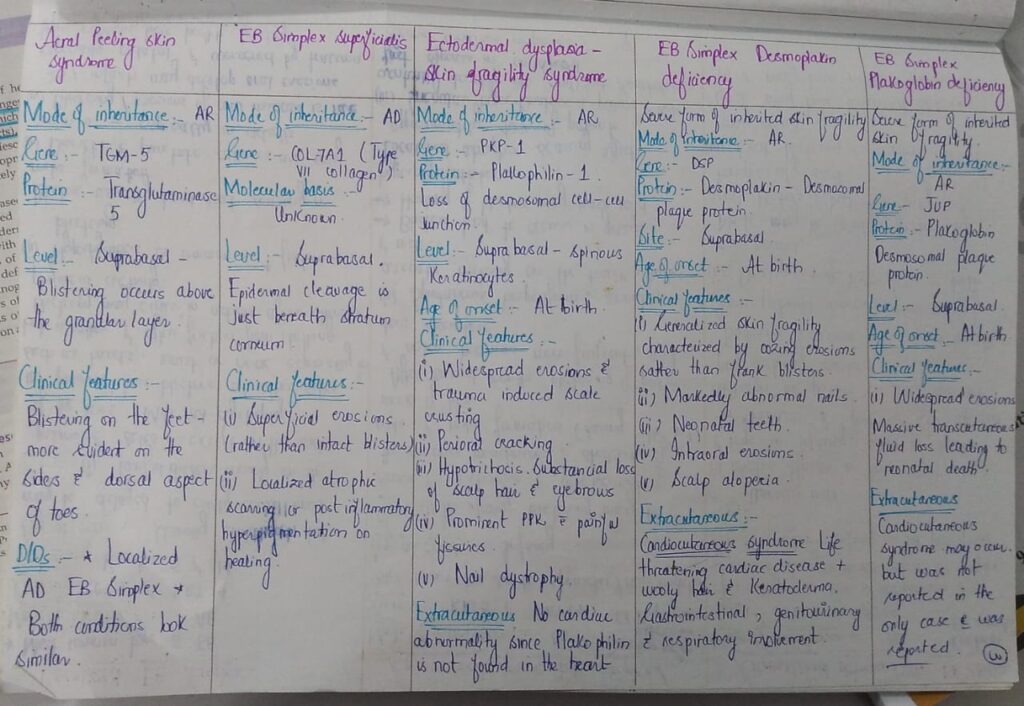
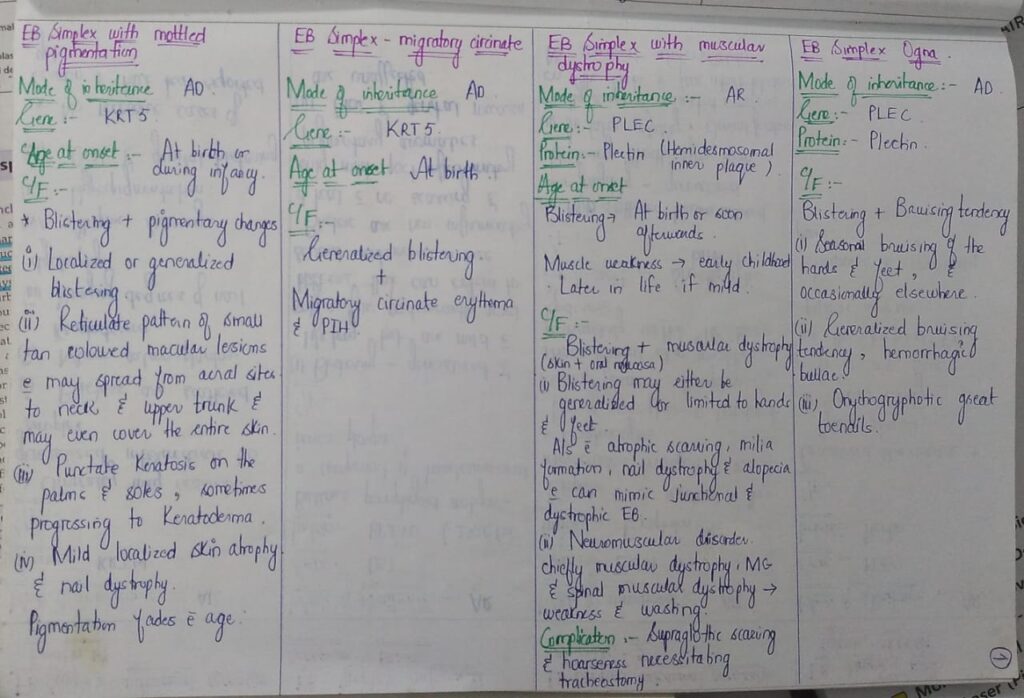


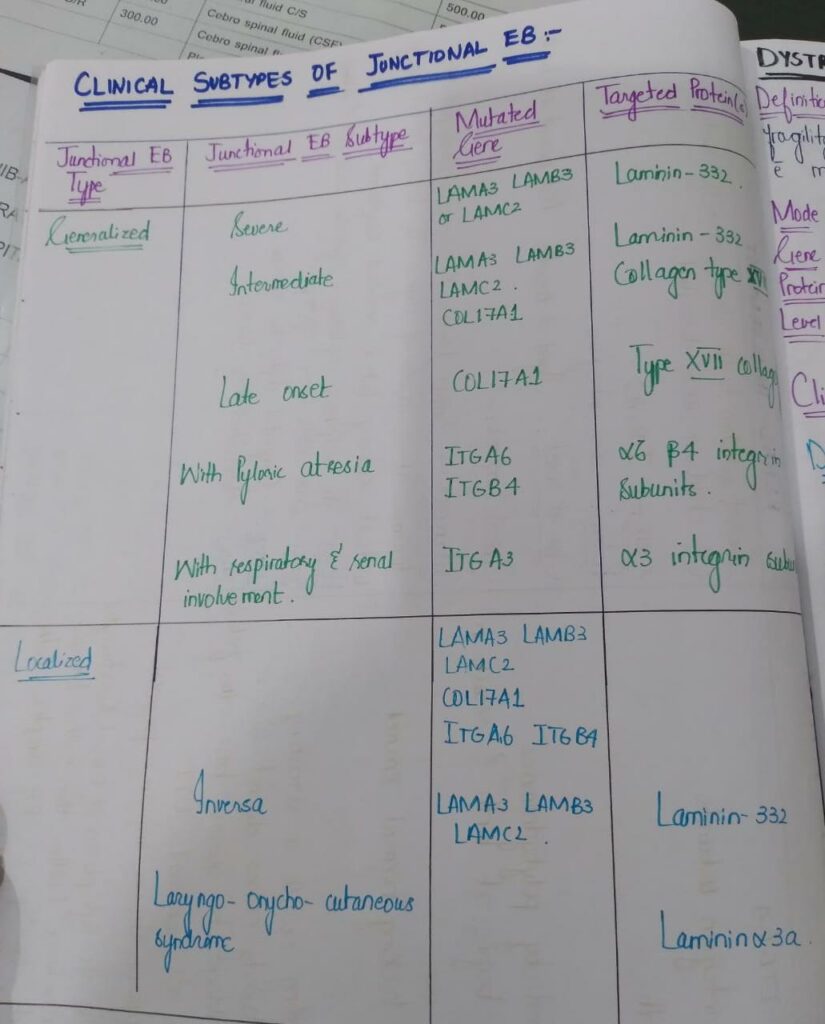


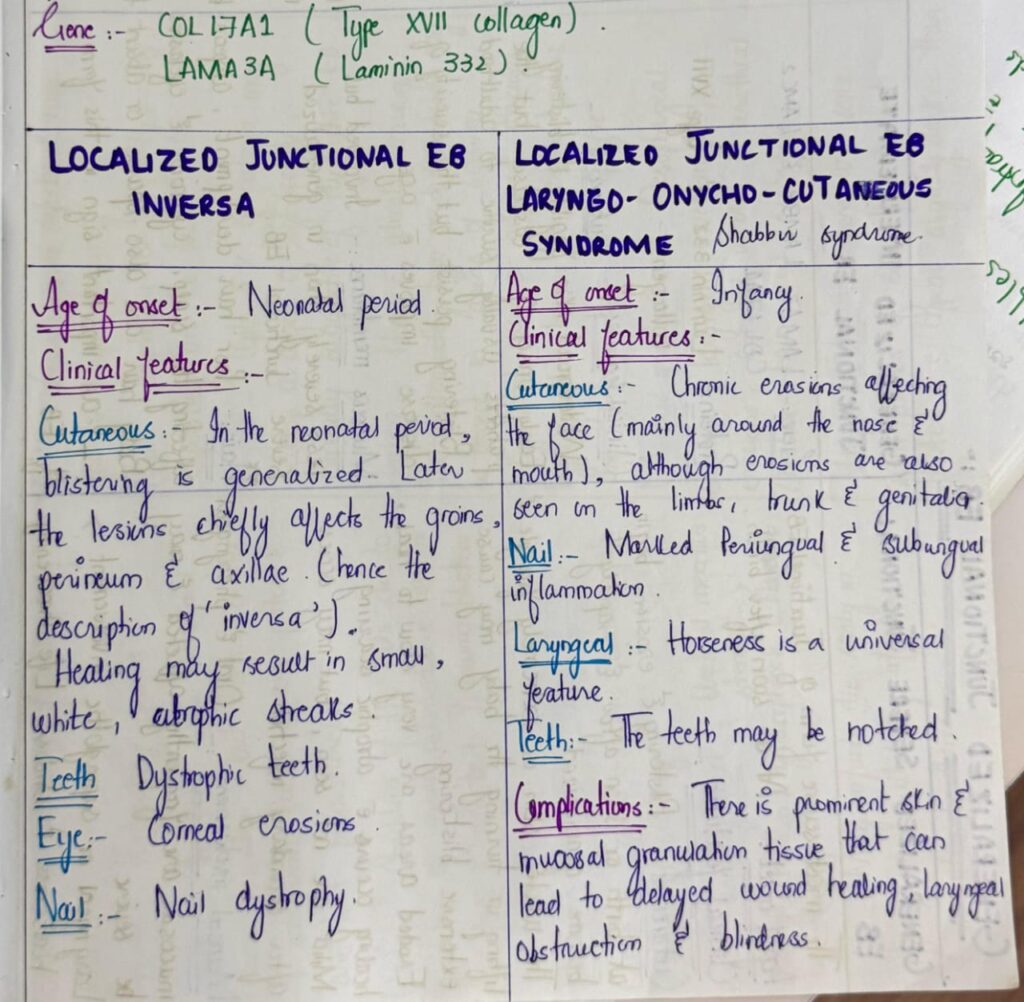






*Important note* EB is a really imp chap from both theory and viva exam point of view. U must revise it again n again to become fluent in answering the questions. Listen to above voice notes and then revise from tables which i have shared and then practice by solving mcqs. ETAS has a very useful mcq pool esp genetics, which makes concept clear.