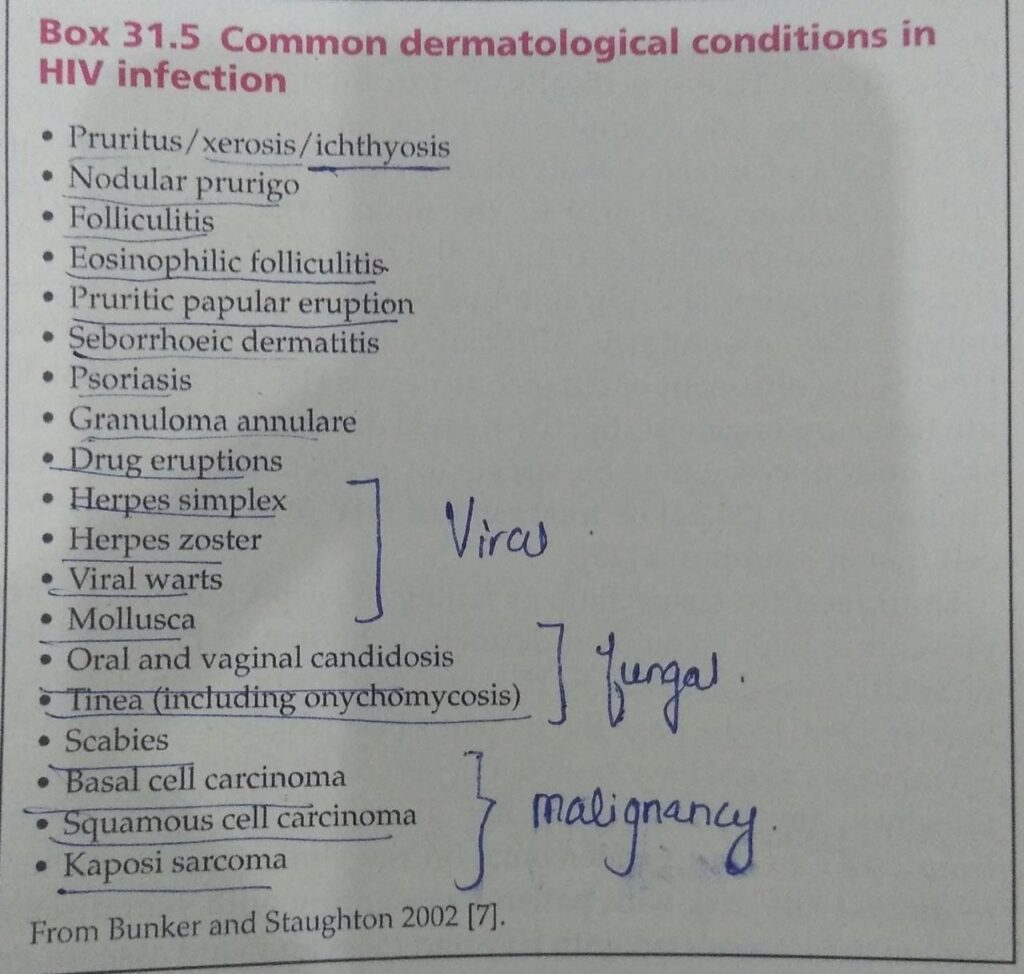
#pearls topic is HIV.
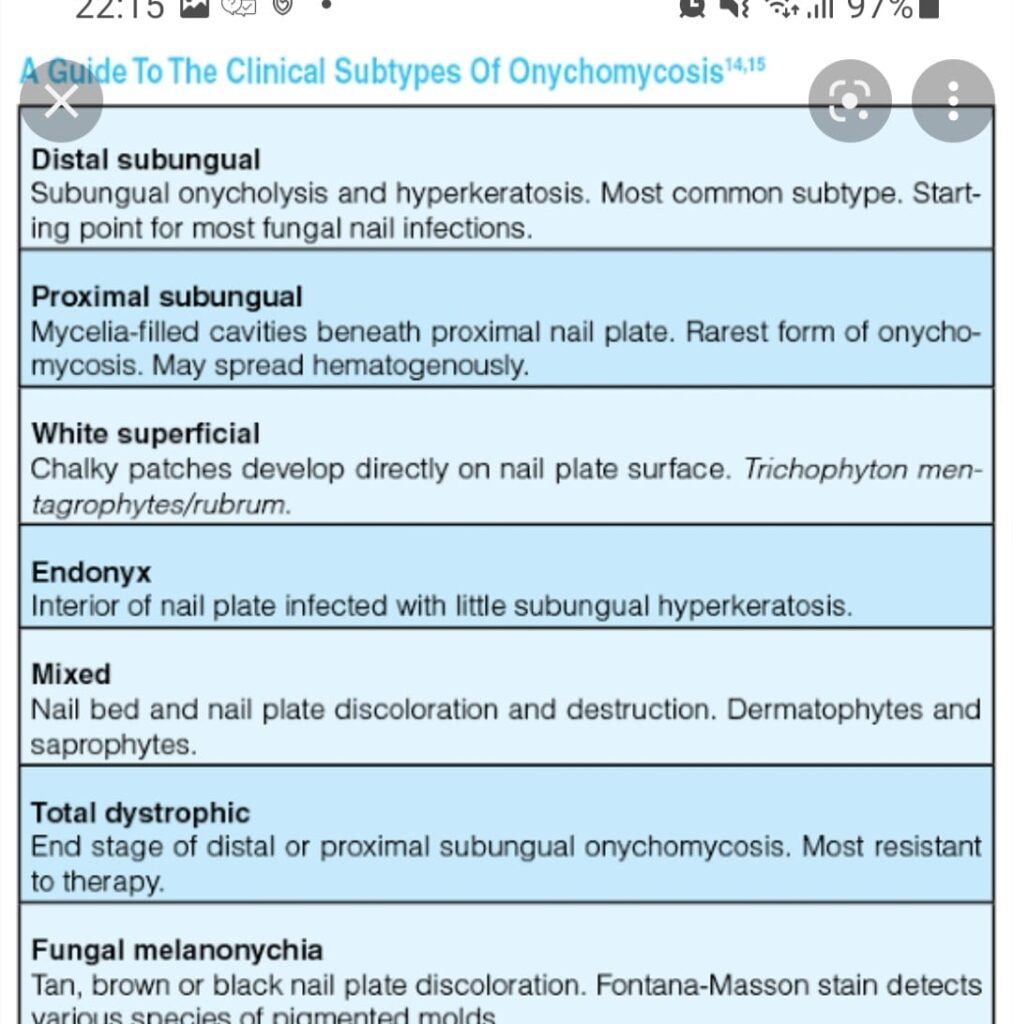
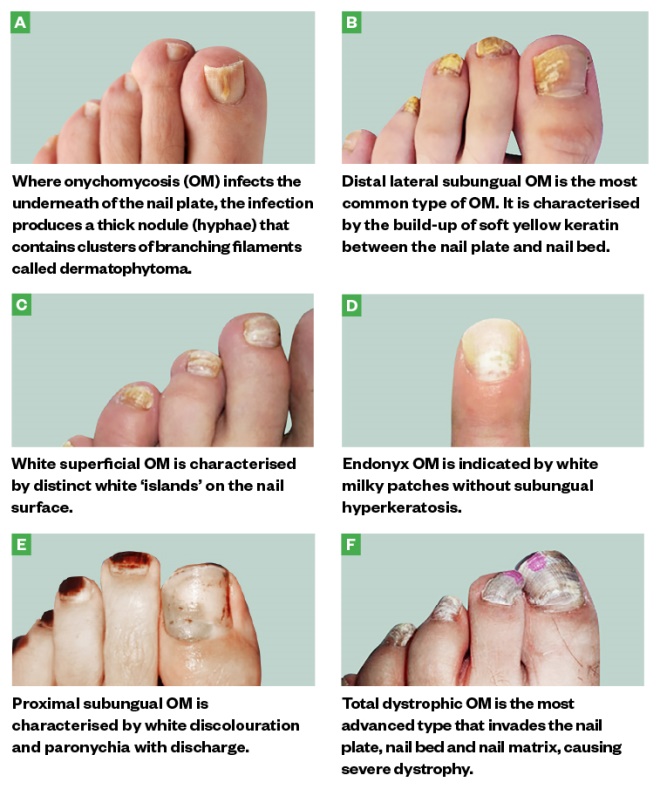
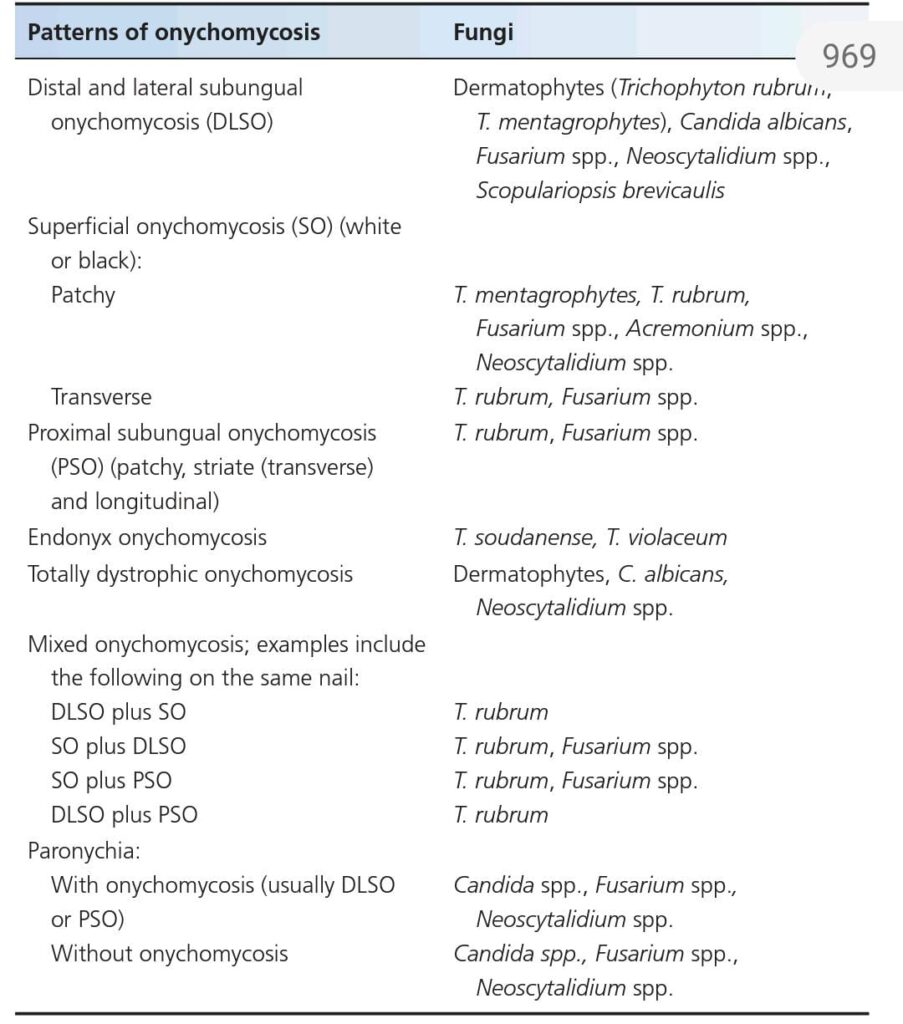
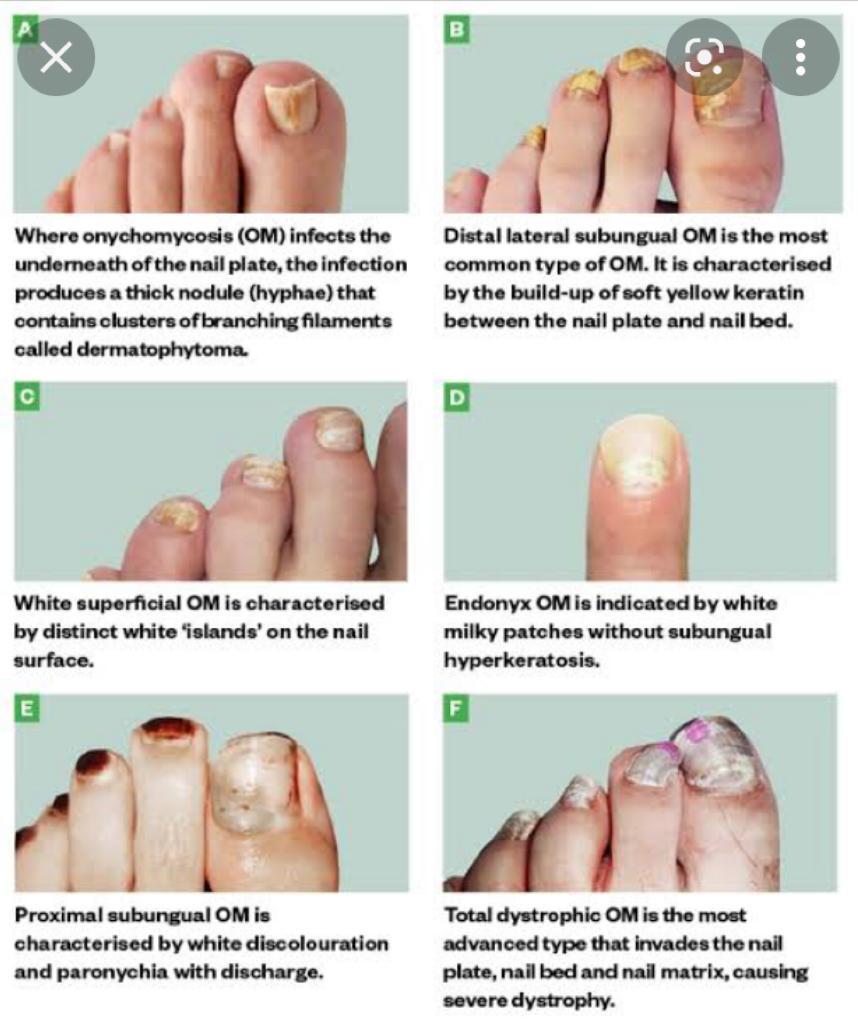
1-Most common pathogen to cause onychomycosis…..T.ruburm
Treatment of fungal infection… Same as in Non HIV. Oral terbinafine is safe.
2-Stain used for cutaneous histoplasmosis is Gomori methenamine silver stain
Stain used for systemic histoplasmosis is wright stain.
3-Cryptococcal infection …stain used is mucicaramine or tznack smear
Poor progsis if CNS involvement .
4-Leishmaniasis is difficult to treat compared to the one in normal person.it is associated with rheumatoid nodulosis.
5-Crusted scabies may b localized to sole or genitalia. On histo , eccrine ductal and follicular mucinosis can be seen.
6-kaposi sarcoma,a spindle cell tumor,risk increase if topical tacrolimus used in HIV.In children or non HIV person transmission is by saliva.
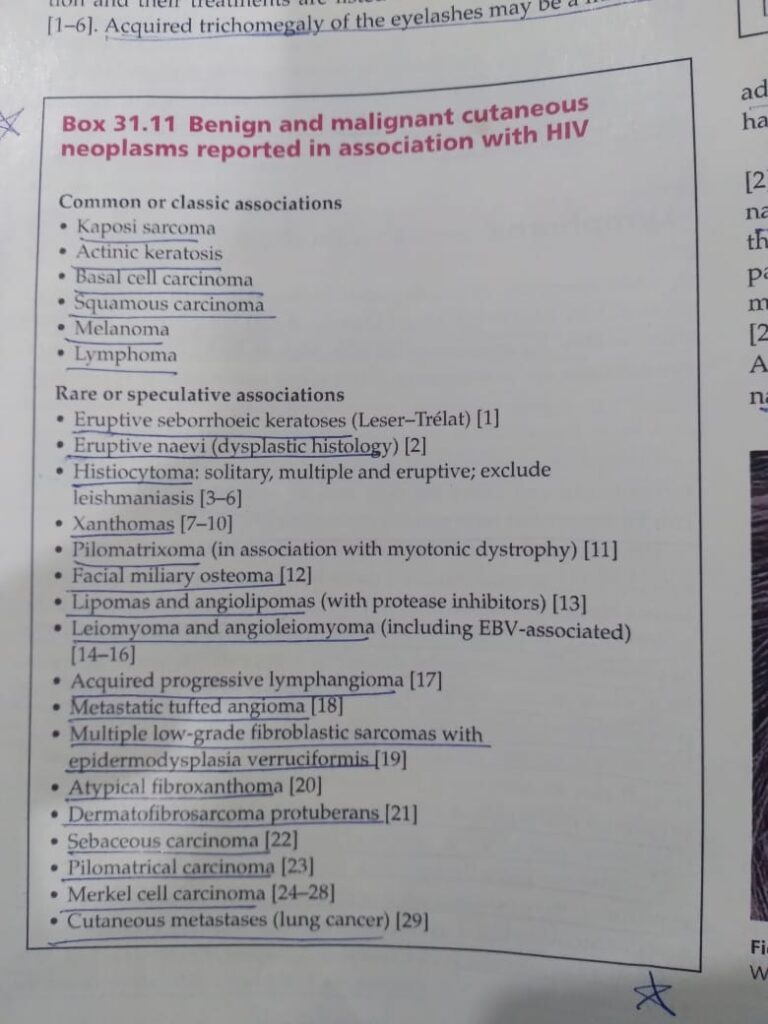
7-ratio of SCC:BCC 1:7
8- long term voriconazole therapy ,associated with multiple BCC.
9-melanoma ,a non AIDS defining cancer, has poor prognosis if CD4 count is low
10-most common BCC is superficial spreading type,treated with topical imiquimod
11- hodgkin disease with mixed cellularity and lymphocyte depleted ,more common in HIV.
12-most common lymphoma is NHL.
13 T.ruburm ,most common cause of onychomycosis
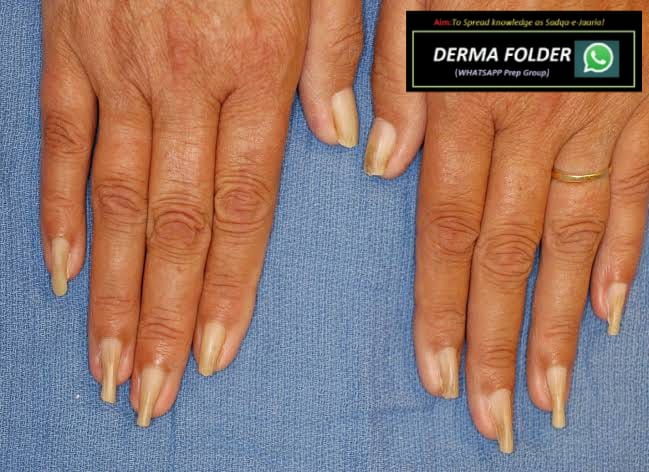
14- grey nail seen at CD4 count< 200 ×10⁶/L.
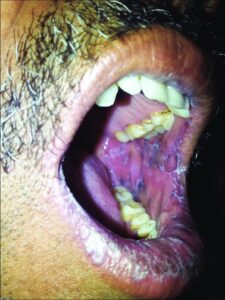
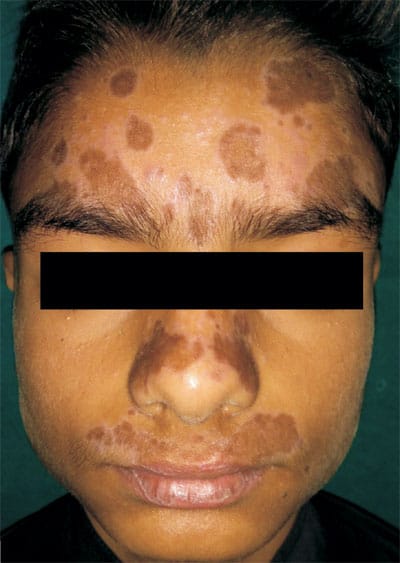
15-Oral hyperpigmentation is sign of low CD4 count (<200) .
16-If pt has hairy cell leukemia, 75% chance to develop AIDS with in 2 to 3 years.
17-concrum oris(noma), seen in malnourished HIV infected children.
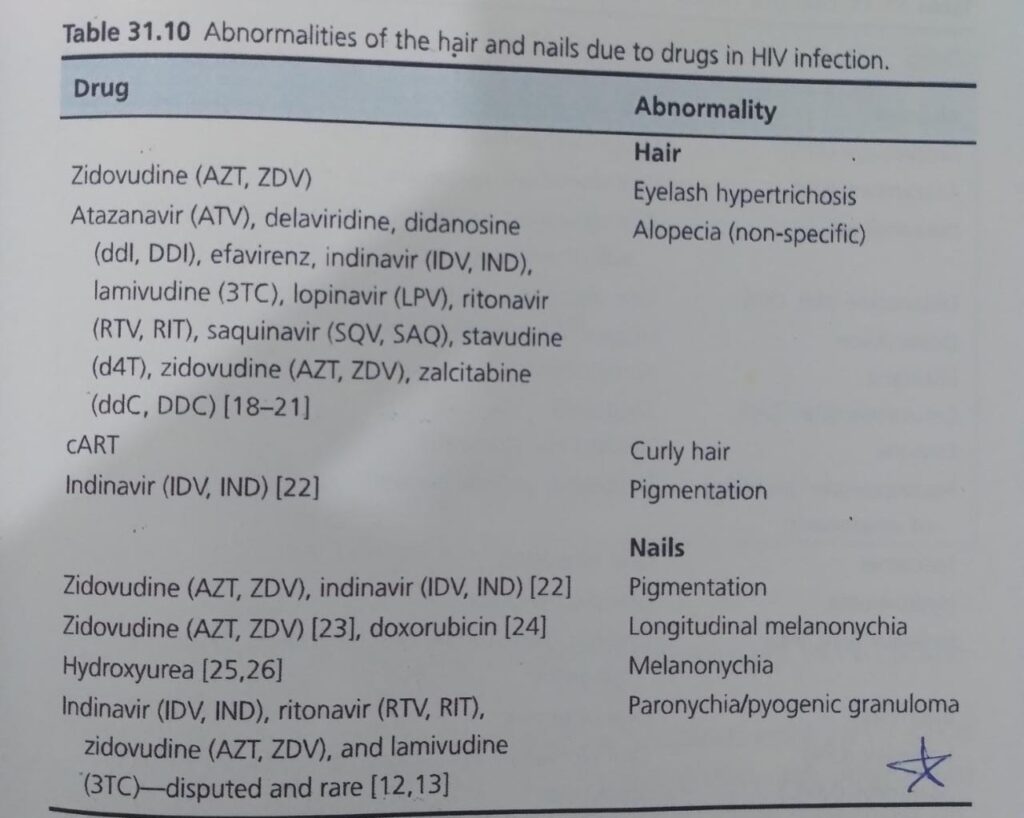
18- hydroxyurea , cause melanonychia.
19- indinavir and zidovudine cause hair and nail pigmentation
20- foscarnet … side effect :Penile ulceration and eosinophilic folliculitis