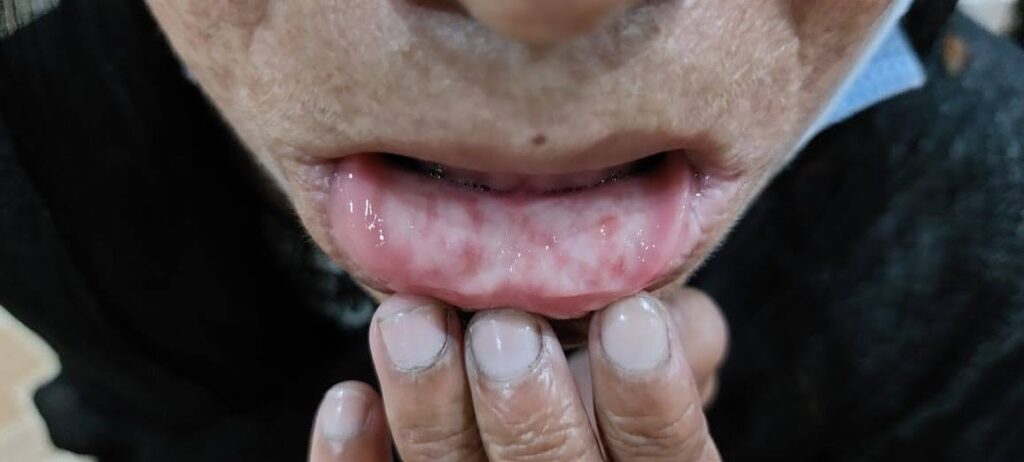
In exam, if there is a short case of lipoid proteinosis we do not give dds. We simply say our provisional diagnosis is lipoid proteinosis.
If the examiner asks what other dds can we keep by juz looking at the scars then u may mentions other dds of pock like scars
Erythema multiforme:
Erythema nodosum:
Sporotrichosis:
Lymphedema:
Granulomatous Cheilitis:
Jessner's lymphocytic infiltrate:
Lymphocytoma cutis
Granuloma faciale
PLE
Epidermolysis bullosa:
Lentiginosis:
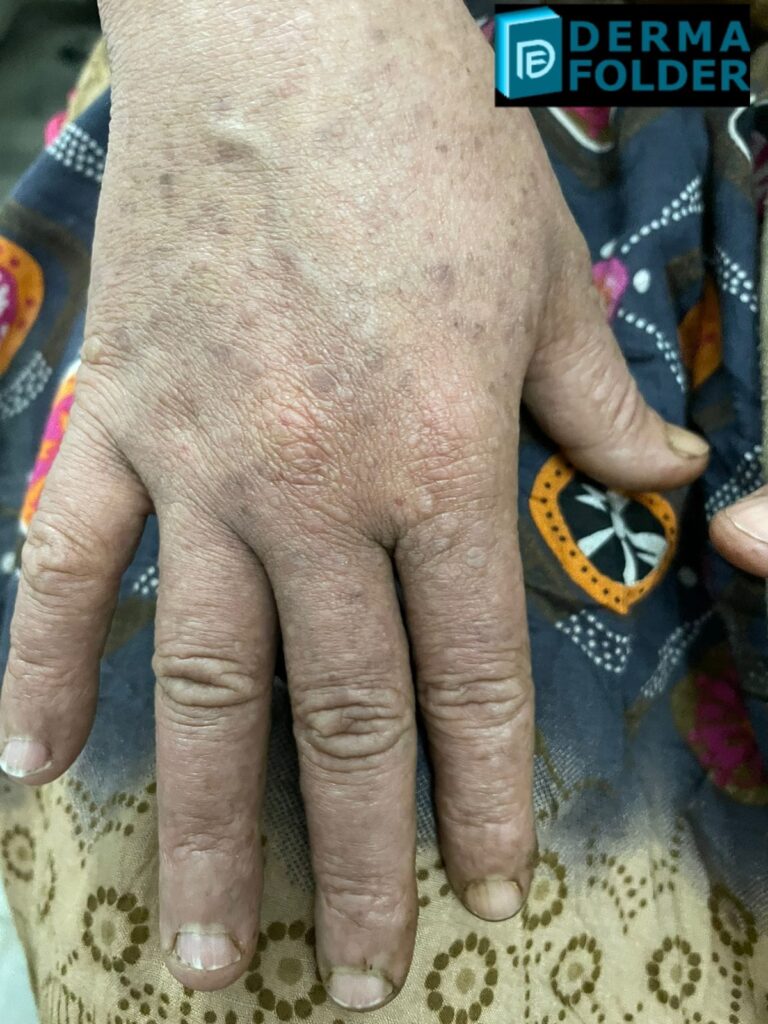
Arsenical keratosis:
EDV. Epidermodysplasia Verruciformis:
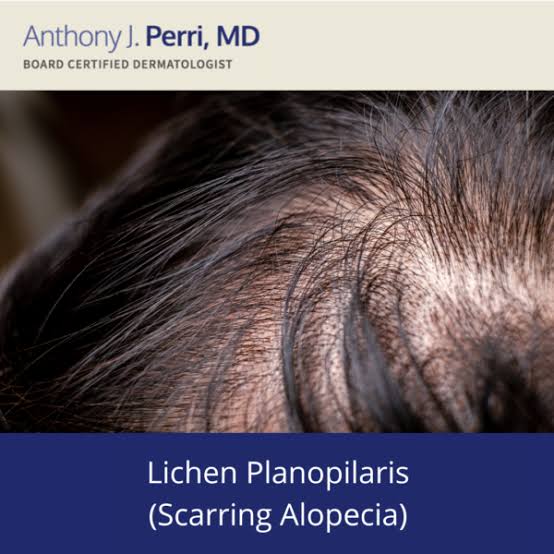
Alopecia:
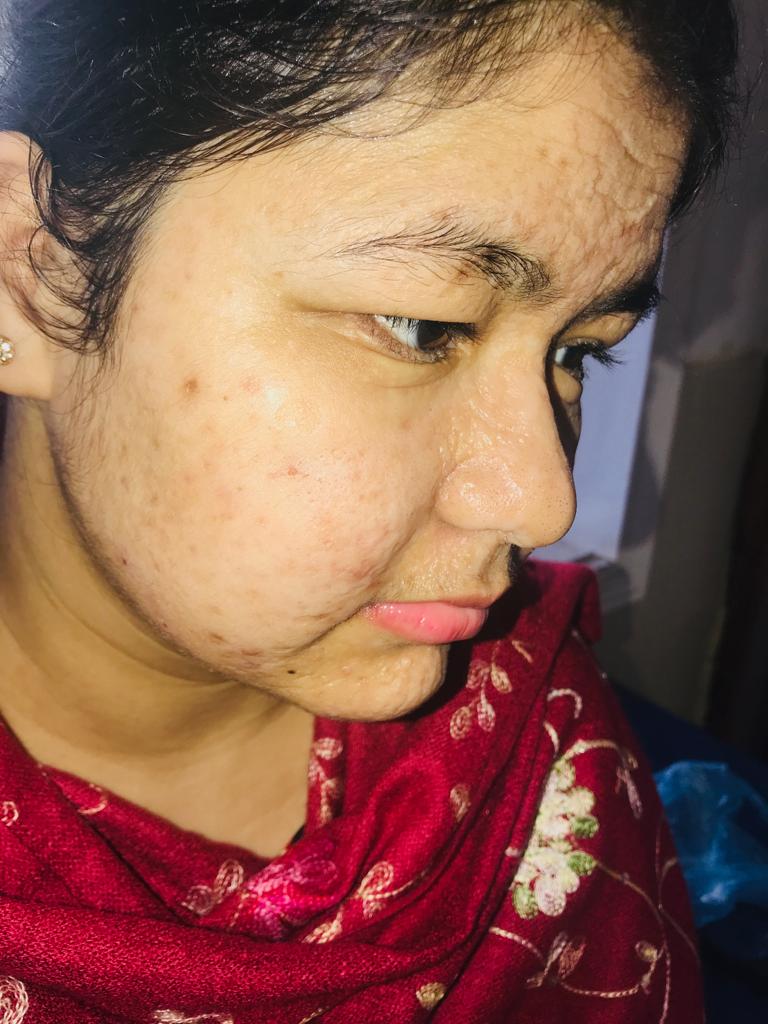
Amyloidosis:
🔰 Important note
In a short case of amyloidosis, examine the skin from head to toe, starting from the region of command.
In exam we had a pt with typical lesions of papular amyloidosis on shin bilaterally but she had lesions of macular amyloidosis on her back and shiny nails secondary to chronic pruritis.
So take home lesson is to look for lesions of all types of amyloidosis in the same patient and for the signs of associated features too.
Acrodermatitis enteropathica:
Porokeratosis:
Hidradenitis suppurativa:
Portwine stain/ hemangioma:
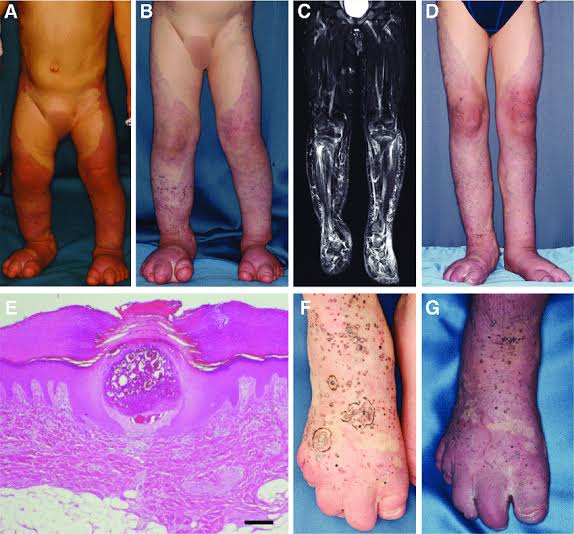
KTS
Lichen planus:
Hypertrophic LP👇🏻
Prurigo nodularis
RPCs
Leishmaniasis:
Rosacea:
Juvenile xanthogranuloma:
LCH:
Calcinosis cutis:
Sweet syndrome:
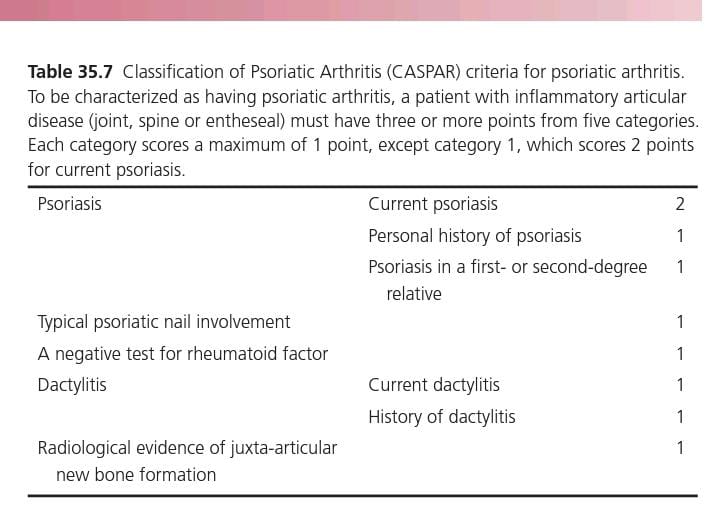
Reiter's arthritis/ Reiter's syndrome:
Relapsing polychondritis:
Darier disease:
Hailey hailey disease:
Kaposi sarcoma:
🔰 IMPORTANT
Kaposi sarcoma is an important short case which frequently comes in exam.
Scroll through the images in google if u dun get a chance to examine a patient bcoz u never know wot cases u get in ua final exam
Ichthyosis:
Papulonecrotic tuberculid:
Lichen scrofulosorum:
Variants of KP👇🏻
Melanoma:
Incontinentia pigmenti:
🔰This case came in our exam as a short case👆🏻
ILVEN – Inflammatory linear verrucous epidermal naevus
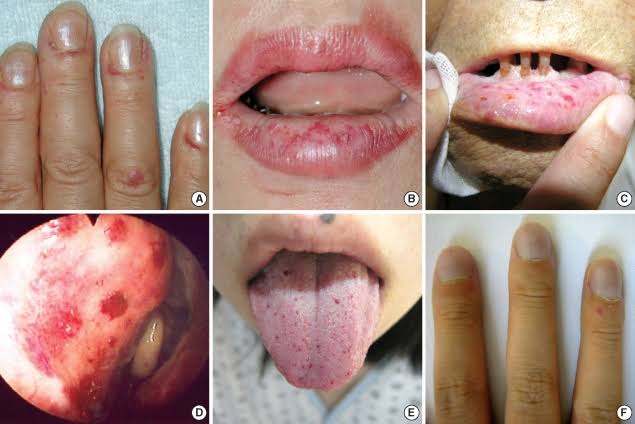
Hereditary hemorrhagic telangiectasia:
Palmoplanter keratoderma:
Morphea:
Linear morphea👇🏻
🔰 IMPORTANT👇🏻
Morphea is a very imp opd and esp imp exam case which is a must to come in exam. So u must practice it really well
LSA
Hypopigmented patch/patches:
Ehler danlos syndrome:
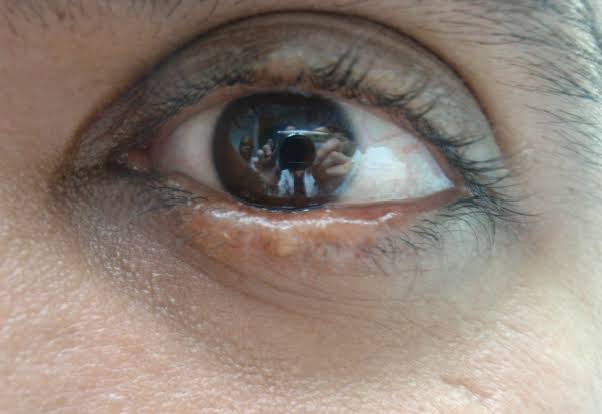
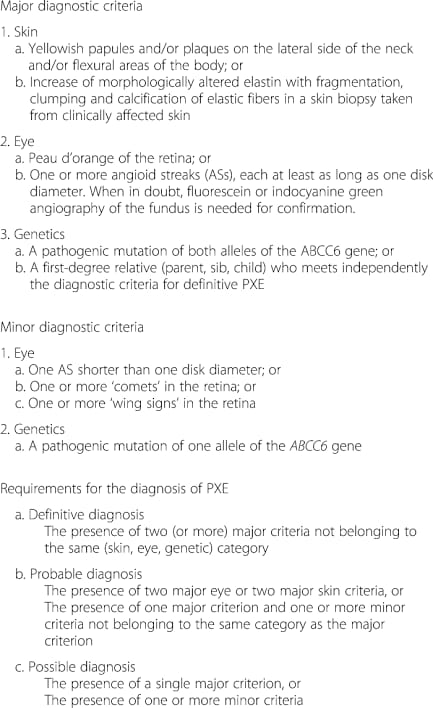
Pseudoxanthoma elasticum:
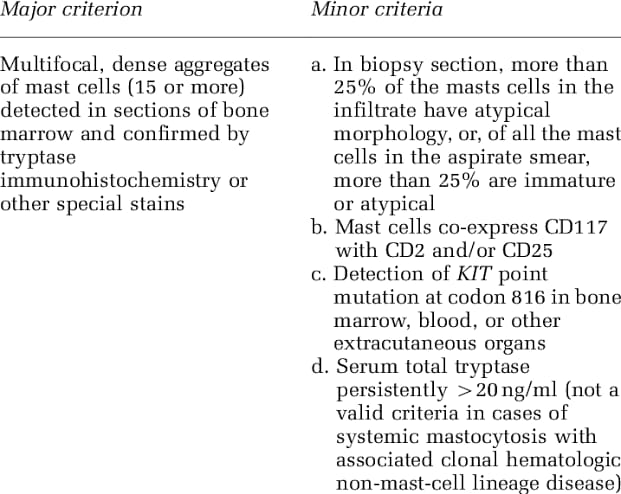
Urticaria pigmentosa:
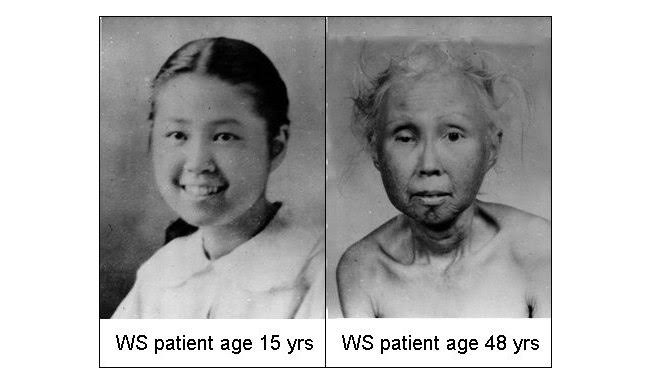
Werner syndrome:
Xanthomas:
Cutis verticis gyrata:
Cutaneous Lymphoma:
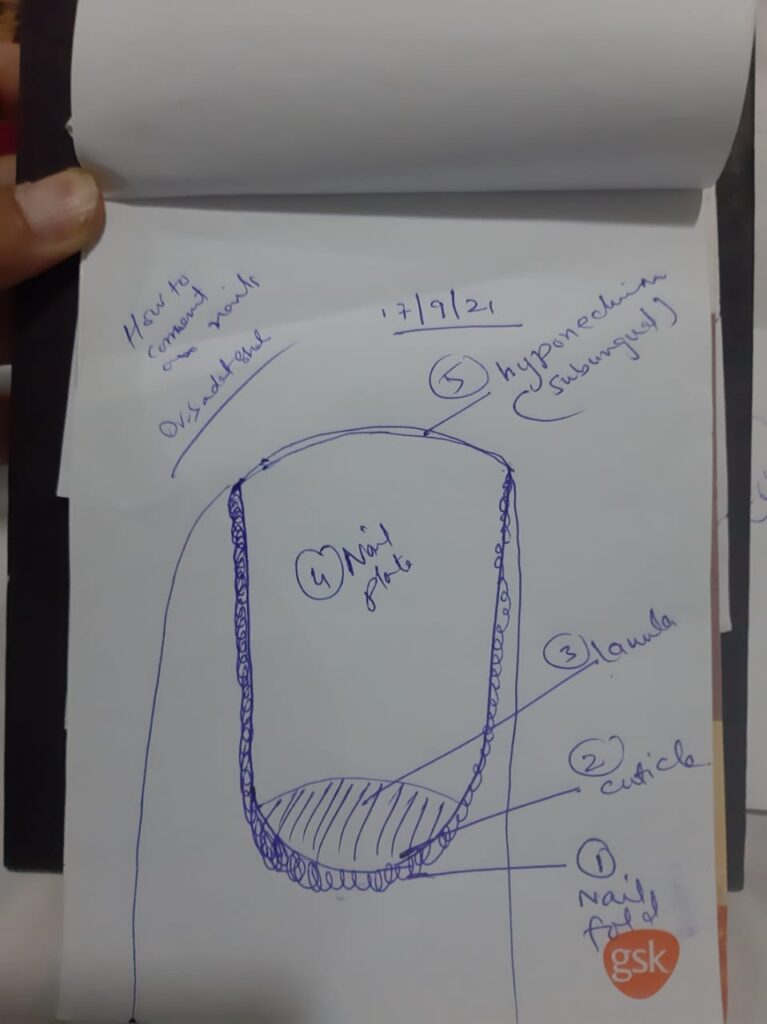
Nail examination by worthy Dr Saadat sb👆🏻
Lupus panniculitis:
Herpes zoster:
Eczema herpeticum:
Hypomelanosis of Ito:
Syphilis:
Kindler syndrome:
Important tip for short case preparation:
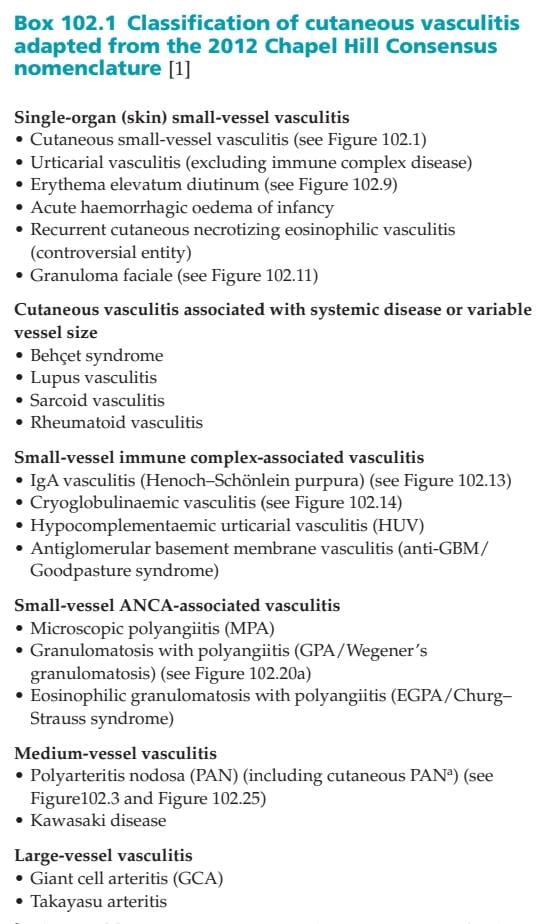
Vasculitis:
Leprosy:
Dds
Leprosy
Hypopigmented MF
Hypopigmented sarcoidosis
Investigations ..
Slit skin smear
Skin biopsy
Serology to pgl 1 antibodies.
To start treatment
CBC
LFTs
RFTs
Eye examination.
Management..
MDT along screening of family .
Multibacillary
Stop infection with chemo
Treat complications and reactions
Educate patient and rehabilitation socially and psychologicaly.
WHO multidrug therapy .
Day 1
Rifampicin 600mg
Dapsone 100mg
Clofazamine 300mg
Day 2 to 28
Clofazamine 50mg
Dapsone 100mg
For 12 months ..
Screening of close contact as well as giving prophylactic dose of Rifampicin to close contacts
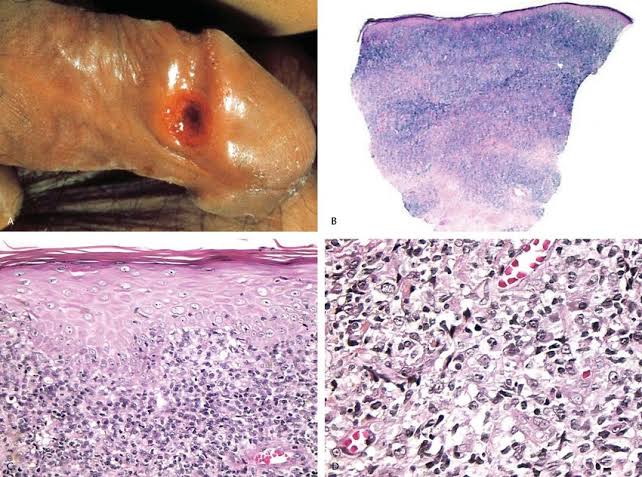
Pagetoid reticulosis:
This 25 year old man presented with these lesions from last 5 years and are gradually increasing in size.
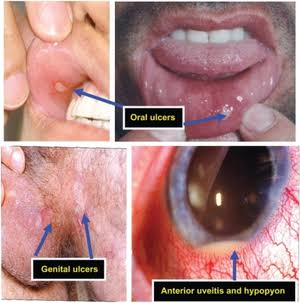
Adamantiades behcet disease:
DFSP:
Dds
Dermatofibrosarcoma protuberance
Lobomycosis
Keloid
EBA:
Multicentric reticulohistiocytosis:
Ichthyosis hystrix:
Steatocystoma multiplex:
Test:
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.