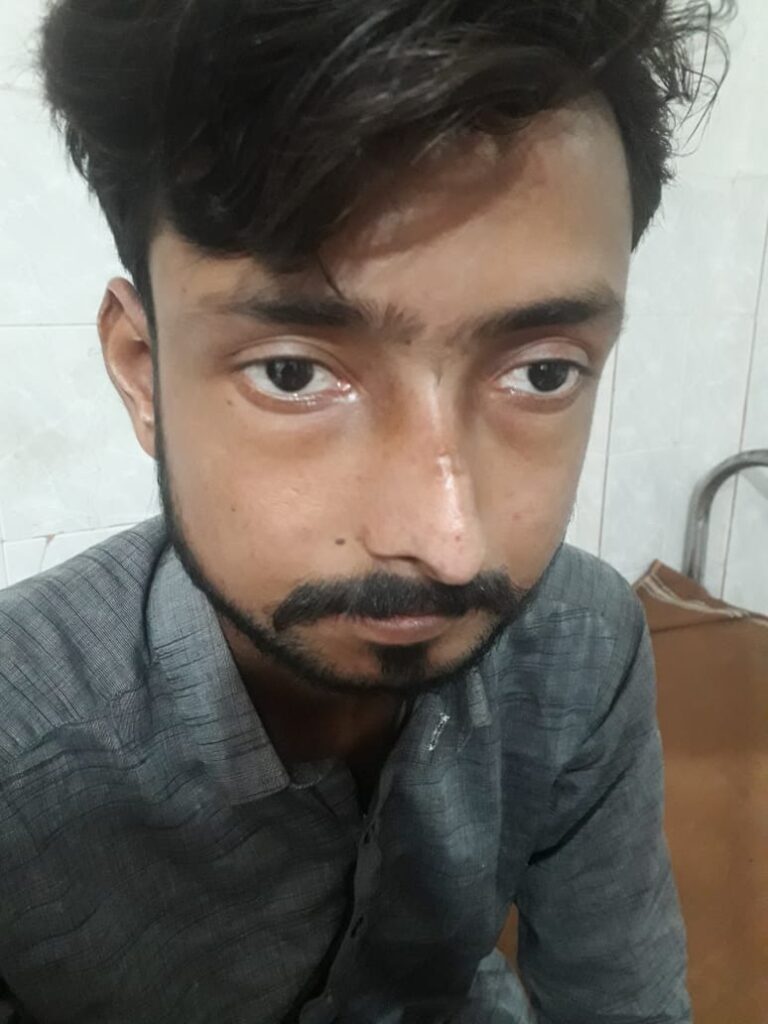
What are the eye changes in systemic sclerosis??*
– start from outside… eyelid stiffness, eyelid telengiectasis
– cataracts
– glaucoma
– keratoconjuctivitis sicca
– optic neuropathy
– orbital fat atrophy
What are the git findings ??
Remember findings from top to bottom, you will never forget
- Start from mouth i.e microstomia & icrocheilia ( this is dec in mouth width)
- Xerostomia
- Then comes teeth, enamel is damaged
- Dysphagia/ regurg
- Gastroparesis
- Small bowel dysmotility
- Large bowel diverticulosis
- Ano rectum… this is 2nd most common site affected after oesophagus, internal anal sphincter is involved
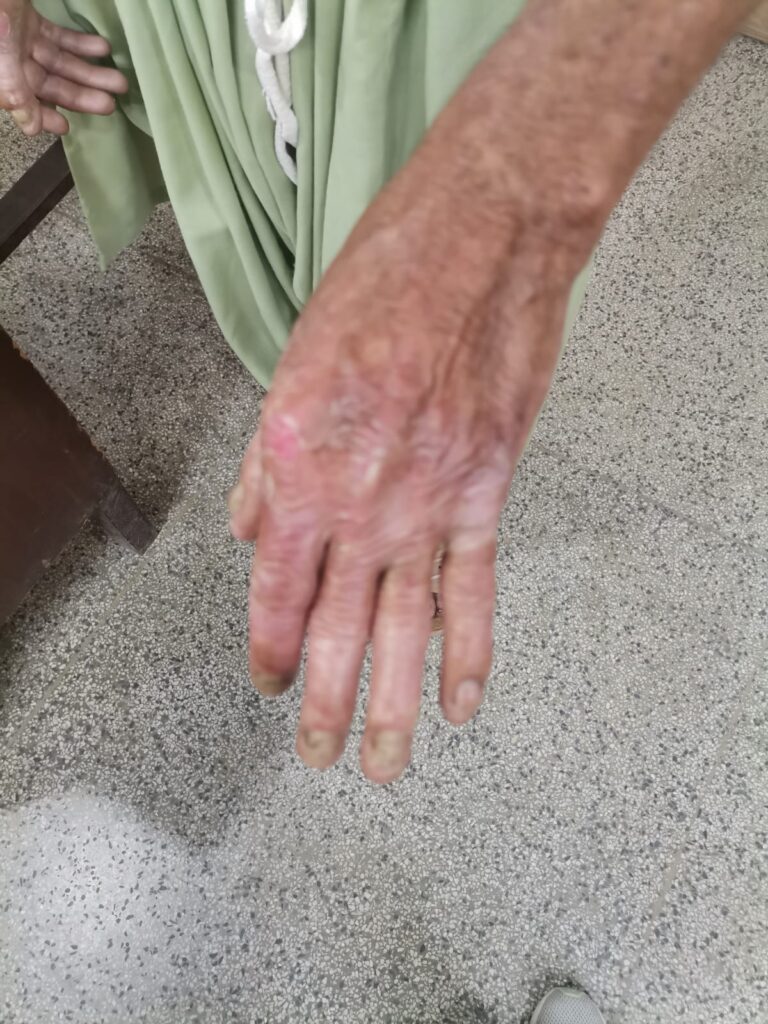
What are the bone changes in systemic sclerosis ?*
– phalangeal resorption
– erosive arthropathy ( pestle and mortar deformity)
– flexion deformities
– acro osteolysis
– joint space narrowing
-severe resorption of 1st carpometacarpal joint with radial subluxation and this is characteristic finding…
– calcinosis
What are soft tissue changes ?*
– subcutaneous and periarticular calcification
– atrophy of finger tips
What are the ecg findings in systemic sclerosis ?*
ST-T changes
– conduction abnormalities like LBBB, first degree AV block, prolonged QT, SVT, VT
What are the echo findings in systemic sclerosis?
*
diastolic dysfunction
valvular regurgitation
Right ventricular pathology
DETECT study
A non invasive method to tell us when to go for invasive right heart catheterization.
🔅Step 1
Calculate a score by measuring 6 parameters
-fvc predicted /dlco predicted
-telengiectasia yes or no
– anti centromere antibody yes or no
– right axis deviation on ecg yes or no
– serum urate level
– pro bnp level
( easy to remember 3 have yes or no, and 3 are values)
If the score is more than 300 then go for echo
🔅Step 2
You see right atrium area in cm2,
TRJ (tricuspid regurgitant jet) velocity in m/s and step 1 total risk score
If its more than 35, then right heart catheterization is recommended..
HSCT considered in SSc when 👇🏻
Disease is rapidly progressive
Severe visceral involvement esp pulmonary involvement
Unresponsive to treatment
🔰 IMPORTANT 🔰
Systemic sclerosis is a very imp long case which always comes in exam, isolated or as a part of MCTD.
So its imp to know every aspect of it.
Like other long n short cases, examiner already makes his mind in the first 10mins after listening to ua history so its critically imp to have a firm grip over history taking and then on the examination.
Ua body language says it all about how many patients u have examined.
So practice as much as u can, ofcourse with a timer on ua bedside coz without time management even the best candidates face the bitterness if failure.
Happy learning😊
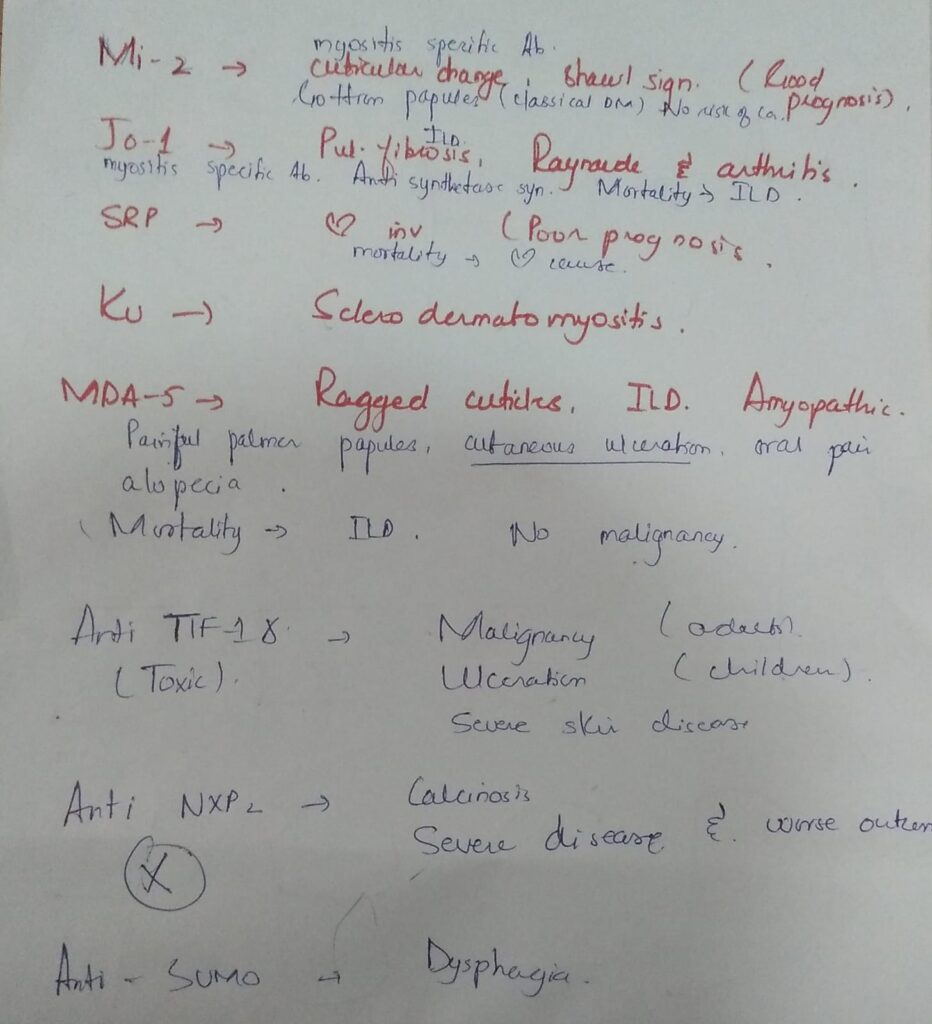
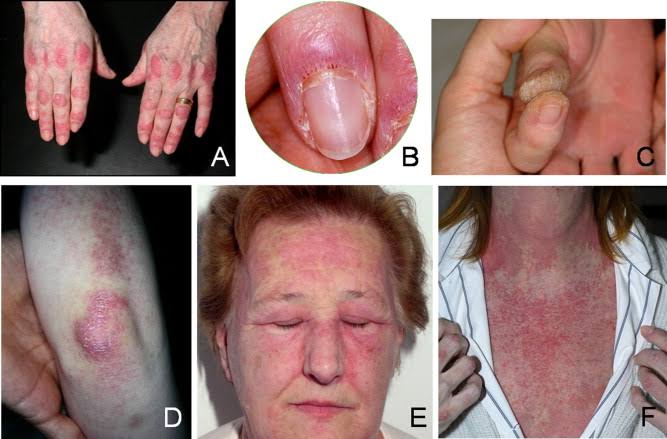
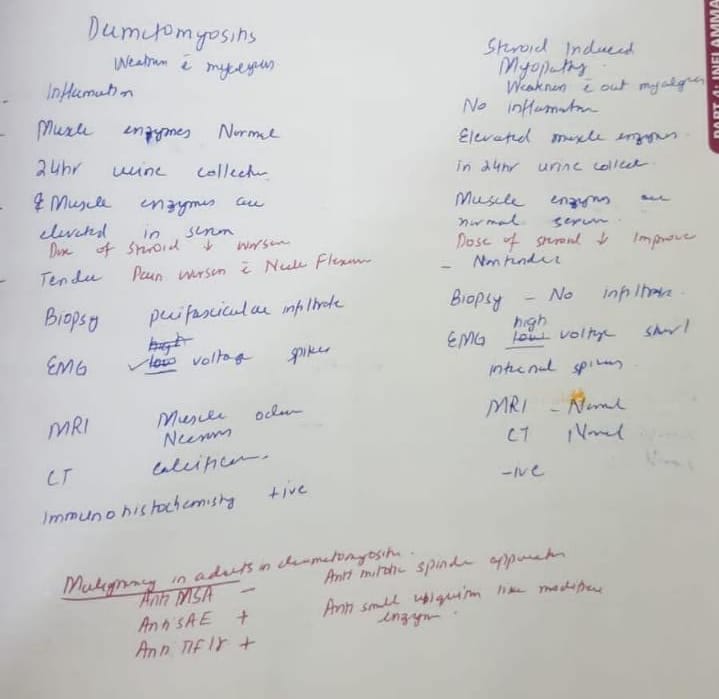
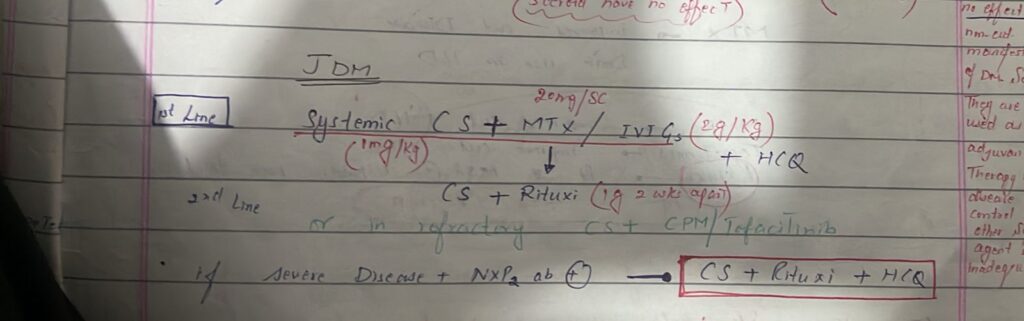
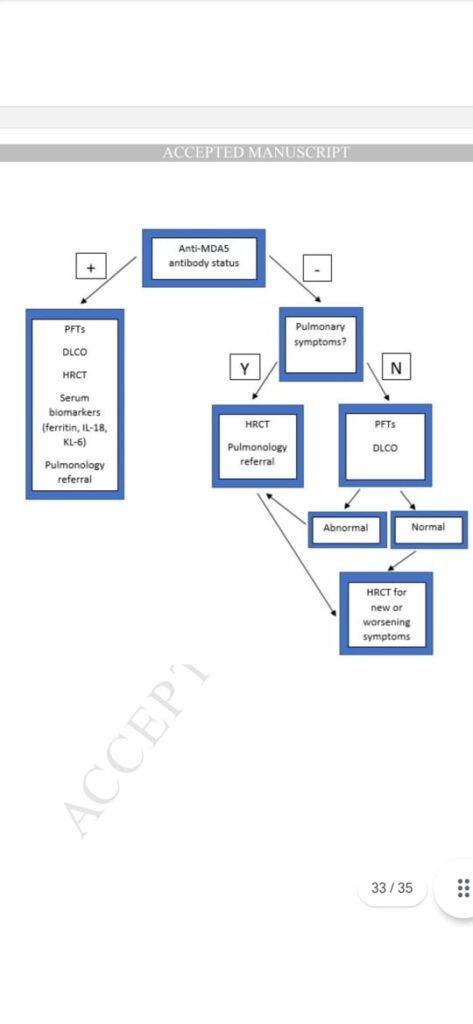
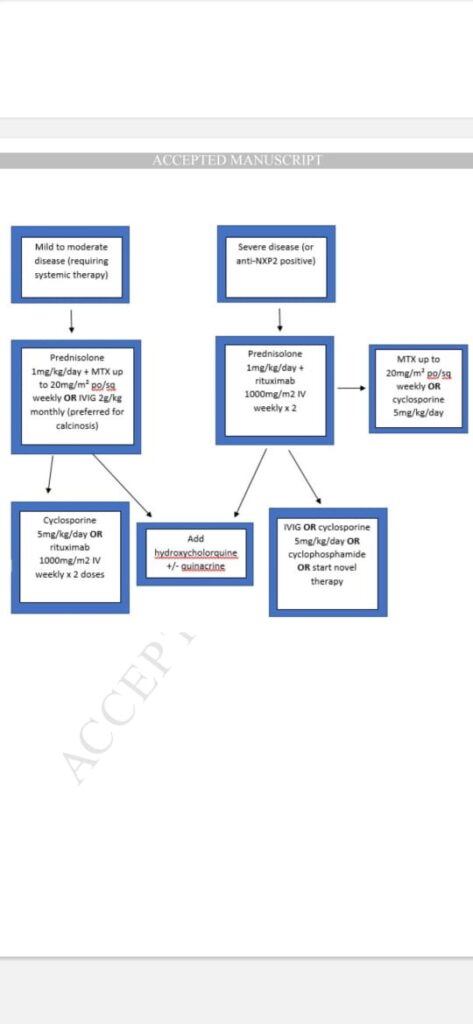
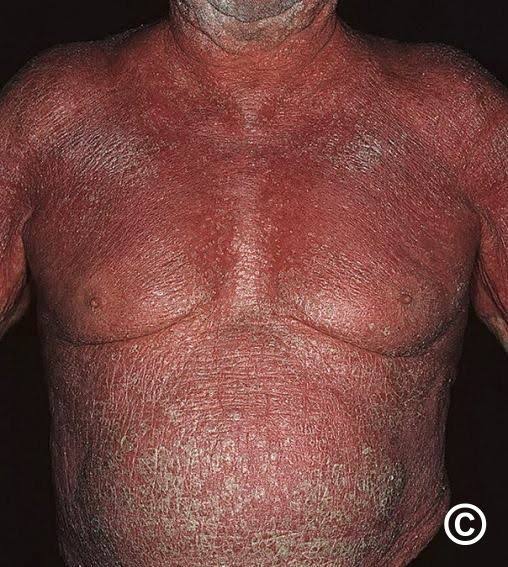
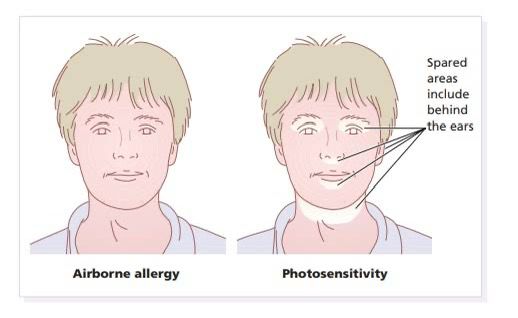
Dermatomyositis