



























Glucocorticosteroids (GCS) are potent anti-inflammatory and anti proliferative agents widely used .
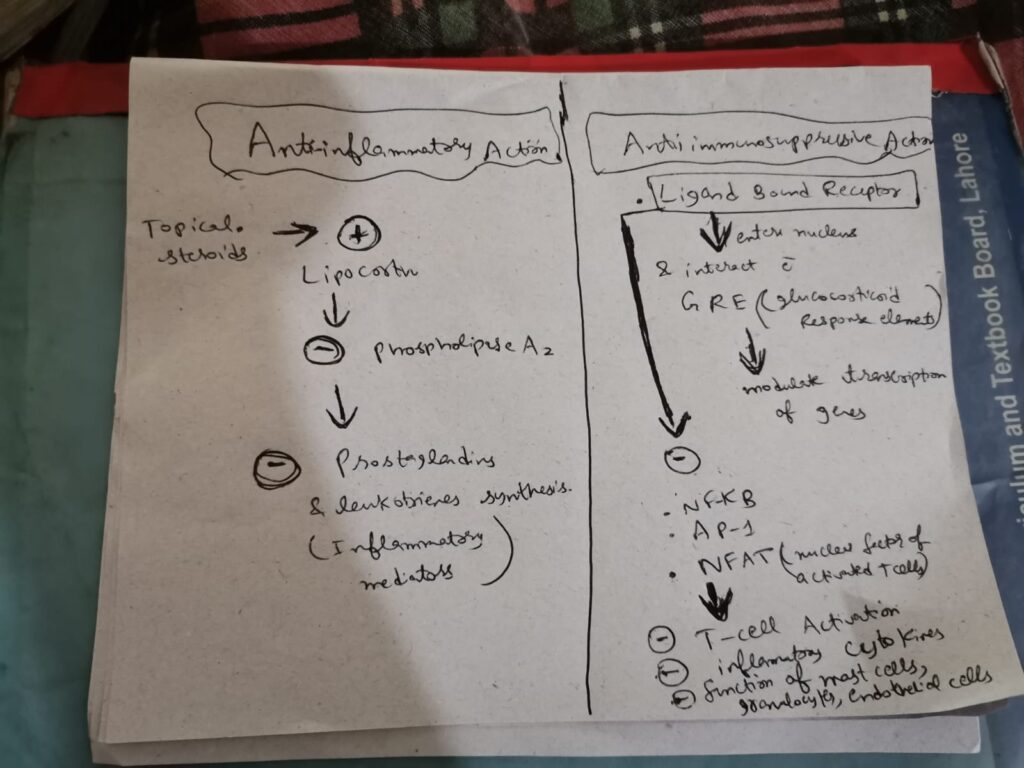
 Anti-inflammatory effects of GCS have been attributed to lipocortin
Anti-inflammatory effects of GCS have been attributed to lipocortin
antiproliferative effects are mediated through the inhibition of several immune functions through a down-regulation of cytokine gene expression.
Effect lymphocytes adhesion to endothelium
VASOCONSTRICTIVE EFFECT OF TOPICAL STEROIDS
corticosteroids are transcription factors, that induce synthesis of receptors for vasoconstriction.
Topical steroids work by constricting capillaries and reducing localized swelling and pain.
Inhibit the prostaglandin-mediated vasodilatation
Principles when initiating topical steroid therapy according to body area:
■ ■ Initiate lowest potency to control disease.
■ ■ Topical corticosteroids should be avoided on ulcerated or atrophic skin, and on skin with coexistent infectious dermatoses.
■ ■ Prolonged use of potent agent should be avoided.
■ ■ Treatment with low to medium potency preparations is recommended for large surface areas.
■ ■ Highly responsive diseases will usually respond to weak steroid preparations, whereas less-responsive diseases require medium potency or high-potency topical steroids.
■ Low-potency, ideally nonhalogenated, preparations should be used on the face and intertriginous areas.
■ ■ Very potent steroid therapy, frequently under occlusion, is usually required for hyperkeratotic or lichenied dermatoses and for involvement of palms and soles.
■ Because of the increased body-surface-area-to-body-mass-index ratio and increased risk of systemic absorption, high-potency preparations and halogenated–medium-potency preparations, should be avoided in infants and young children, other than for short-term application.
Dose titration of topical steroids
#Highly potent formulations should be used for short periods (2 to 3 weeks) or intermittently.
#Once disease control is partially achieved, the use of a less-potent compound should be initiated.
#Reduce frequency of application (eg, application only in the morning, alternate-day therapy, weekend use) once disease control is partially achieved.
#Sudden discontinuation should be avoided after prolonged use to prevent rebound phenomena.
#Special guidelines should be followed when treating certain body areas (eg, intertriginous areas) or certain populations (eg, children or the elderly) to prevent the occurrence of local or systemic adverse effects.
#Close monitoring and further evaluation is recommended if systemic absorption of corticosteroids is suspected.
#Use combination therapy when clinically indicated (eg, addition of topical calcineurin inhibitor, tretinoin or calcipotrien)
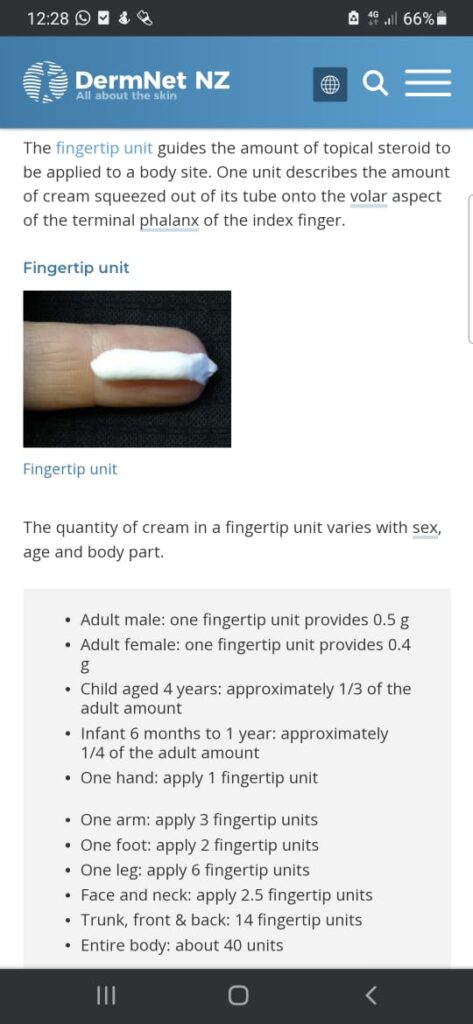
Remember rule of half for FTU application as follows
2% BSA =IFTU= 0.5 grams
And on average it covers 300cm squares area
💊 It is recommended that pts should use no more than 50 grams of super potent steroids/ week
💊 while for potent steroids no more than 100 grams/ week
👶 while in children and babies have a high ratio of surface area to body volume and are more vulnerable to pituitary-adrenal suppression as a result of systemic absorption.